Abstract
This study investigates infant mortality in Uganda, a persistent public health challenge in many developing countries where economic disparities limit access to healthcare. It compares the forecasting performance of three econometric models; Vector Error Correction Model (VECM), Vector Autoregressive (VAR), and Bayesian VAR (BVAR) using annual data on infant mortality rates (IMR), neonatal mortality rates (NMR), GDP, and GDP per capita (GDPP) from 1954 to 2016. Model accuracy was evaluated using Mean Squared Error (MSE), Root Mean Squared Error (RMSE), and Theil’s U-statistic.
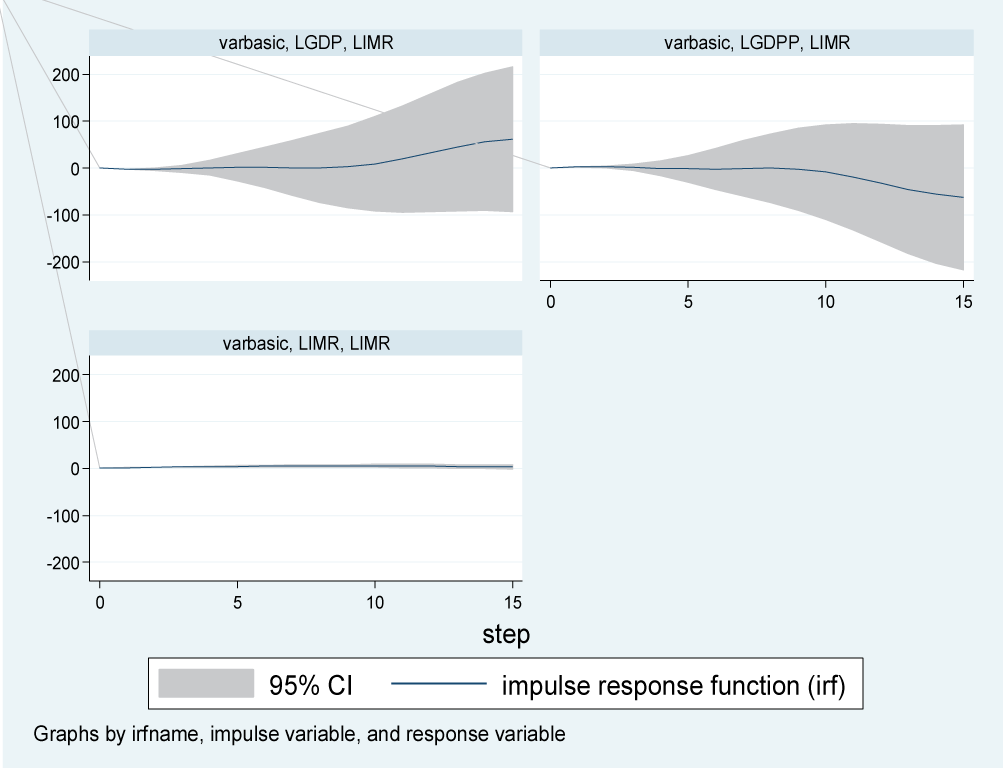
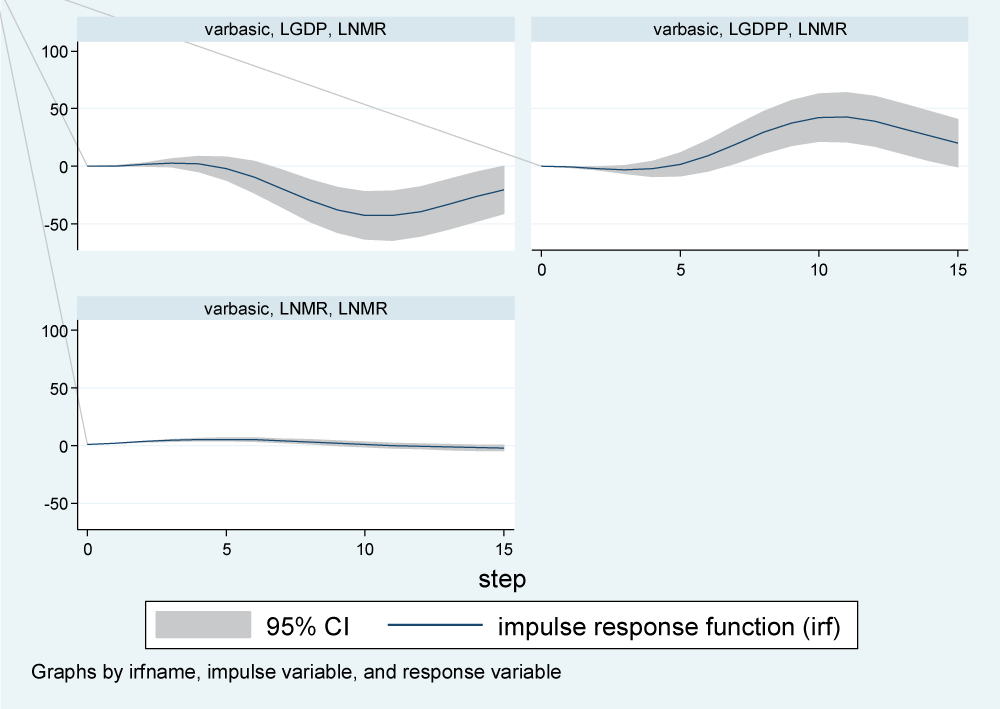
The results show strong long-term relationships among IMR, NMR, GDP, and GDPP. VECM provides the most reliable long-term forecasts, with an adjusted R-squared of 97.7%. Impulse response analysis indicates that GDP increases IMR in the short run, while GDPP exerts a stronger long-term reducing effect. For NMR, GDP has a negative impact, whereas GDPP shows a gradual positive response over time. Granger causality tests reveal bidirectional causality between GDPP and IMR, and a unidirectional influence of IMR on GDP.
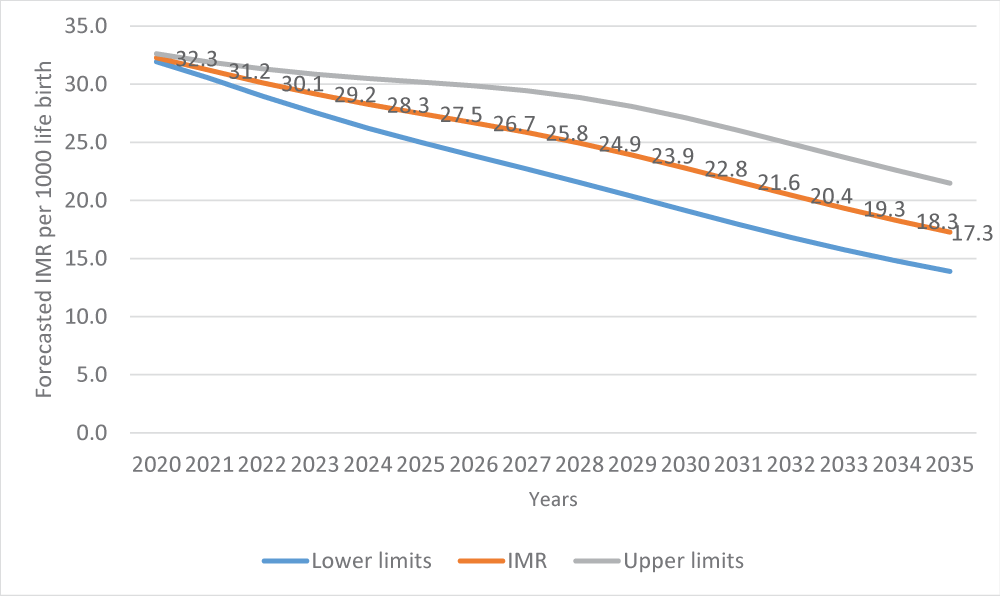
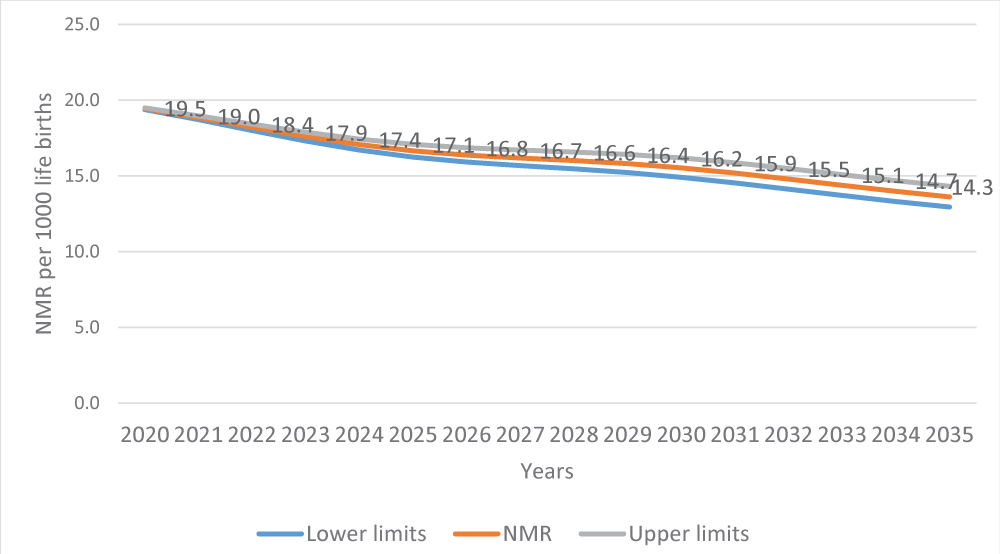
Uganda’s IMR is projected to fall to about 17 deaths per 1,000 live births by 2035, though NMR declines will slow. Policymakers should use VECM for long-term planning due to its superior accuracy and the strong cointegration among IMR, NMR, GDP, and GDPP, while VAR/BVAR can guide short-term monitoring. Because GDPP most strongly reduces mortality, welfare-enhancing strategies such as social protection and employment are crucial. GDP gains should fund maternal and neonatal health, and systems must be strengthened to withstand economic shocks.