IGMIN: We're glad you're here. Please click 'create a new query' if you are a new visitor to our website and need further information from us.
If you are already a member of our network and need to keep track of any developments regarding a question you have already submitted, click 'take me to my Query.'
Welcome to IgMin Research – an Open Access journal uniting Biology, Medicine, and Engineering. We’re dedicated to advancing global knowledge and fostering collaboration across scientific fields.
At IgMin Research, we bridge the frontiers of Biology, Medicine, and Engineering to foster interdisciplinary innovation. Our expanded scope now embraces a wide spectrum of scientific disciplines, empowering global researchers to explore, contribute, and collaborate through open access.
Welcome to IgMin, a leading platform dedicated to enhancing knowledge dissemination and professional growth across multiple fields of science, technology, and the humanities. We believe in the power of open access, collaboration, and innovation. Our goal is to provide individuals and organizations with the tools they need to succeed in the global knowledge economy.
IgMin Publications Inc., Suite 102, West Hartford, CT - 06110, USA
Agentic AI for Ageing Healthcare Systems in Advanced Economies: A Structured Review of Evidence, Institutional Barriers, and a Sociotechnical Implementation Roadmap
Advanced economies face a compounding demographic crisis: populations aged 65 and over will reach 30–40% in several nations by 2050, ageing-related expenditure already absorbs up to 18% of GDP in the most affected economies, and demographic ageing is projected to reduce annual GDP growth by 0.3–1.2 percentage points by 2035. Conventional policy instruments have failed to resolve pressures that include severe long-term care workforce shortfalls across leading ageing economies and per-capita elderly care costs running 3–5 times those of working-age cohorts. This structured narrative review of 81 sources (2020–2025) examines AI’s potential in healthcare, focusing on Agentic AI, autonomous, goal-directed systems capable of coordinating multi-step workflows, to support structural adaptation in ageing health systems. A consistent finding is that implementation outcomes are determined by institutional conditions rather than algorithmic performance, and evidence strength is inversely correlated with intervention complexity. Three conceptual contributions are presented: the Agentic AI Framework (AAF 3.0); a cross-domain synthesis formalising the inverse evidence–complexity relationship; and a phased sociotechnical roadmap integrating governance sequencing, reimbursement reform, and equity safeguards. Short-term productivity gains are documented; macroeconomic fiscal moderation remains empirically unvalidated.
By 2050, one in three citizens in Japan will be over 65, with Italy and South Korea projected to approach 30–40% over the same period [11United Nations, Department of Economic and Social Affairs, Population Division. World population prospects 2024. New York: United Nations; 2024.]. Sustained sub-replacement fertility, including South Korea’s 0.75 total fertility rate (2025 estimate; 0.72 in 2023) [22Organisation for Economic Co-operation and Development (OECD). Health at a glance 2023: OECD indicators. Paris: OECD Publishing; 2023. doi:10.1787/7a7afb35-en], combined with rising longevity exceeding 84 years in Japan and Singapore [33Statistics Korea. 2023 birth statistics. Daejeon: Statistics Korea; 2024.] are driving this transition. Its speed is as consequential as its scale, with demographic ageing that took over a century in France occurring within decades in Japan and South Korea [44World Health Organization. World health statistics 2024. Geneva: WHO; 2024.,55United Nations. World population ageing 2019: Highlights. New York: United Nations; 2019.].
Three structural pressures converge. First, workforce contraction: Japan faces an estimated 250,000 nursing shortfall by 2026 [66Kinsella K, Phillips DR. Global aging: the challenge of success. Popul Bull. 2005;60(1):1–40.], and Italy's long-term care workforce density remains well below the OECD average [77Ministry of Health, Labour and Welfare, Japan. Annual health, labour and welfare report 2023. Tokyo: MHLW; 2023.,88Organisation for Economic Co-operation and Development (OECD). Fiscal sustainability and population ageing: OECD economic outlook. Paris: OECD Publishing; 2023.]. Second, fiscal strain: per-capita healthcare spending for older adults is 3 – 5 times that of working-age cohorts [77Ministry of Health, Labour and Welfare, Japan. Annual health, labour and welfare report 2023. Tokyo: MHLW; 2023.], and ageing alone is projected to add 1.8 – 2.7 percentage points of GDP to public health expenditure by 2060 [88Organisation for Economic Co-operation and Development (OECD). Fiscal sustainability and population ageing: OECD economic outlook. Paris: OECD Publishing; 2023.]. Third, care complexity: multimorbidity and dependency increase coordination demands across already fragmented systems. Ageing also carries human costs obscured by aggregate statistics, including social isolation, solitary deaths, and intensified caregiving burdens that further constrain labour supply [99Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, Brayne C, Burns A, Cohen-Mansfield J, Cooper C, Costafreda SG, Dias A, Fox N, Gitlin LN, Howard R, Kales HC, Kivimäki M, Larson EB, Ogunniyi A, Orgeta V, Ritchie K, Rockwood K, Sampson EL, Samus Q, Schneider LS, Selbæk G, Teri L, Mukadam N. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020 Aug 8;396(10248):413-446. doi: 10.1016/S0140-6736(20)30367-6. Epub 2020 Jul 30. Erratum in: Lancet. 2023 Sep 30;402(10408):1132. doi: 10.1016/S0140-6736(23)02043-3. PMID: 32738937; PMCID: PMC7392084.].
Across the seven most demographically stressed advanced economies, healthcare spending ranges from 6.1% to 16.9% of GDP, and total ageing-related expenditure absorbs between 10% and 28% of GDP in the most affected economies [77Ministry of Health, Labour and Welfare, Japan. Annual health, labour and welfare report 2023. Tokyo: MHLW; 2023.,88Organisation for Economic Co-operation and Development (OECD). Fiscal sustainability and population ageing: OECD economic outlook. Paris: OECD Publishing; 2023.]. The IMF's 2024 Fiscal Monitor projects public health spending in advanced economies will rise by 2.0–3.5 percentage points of GDP by 2050 under baseline scenarios, and by 3.5–6.0 points under adverse trajectories [1010International Monetary Fund (IMF). Fiscal monitor, April 2024. Washington (DC): IMF; 2024.]. Country-level projections are stark: Japan's healthcare expenditure is forecast to rise 55% above its 2023 baseline by 2050; South Korea's is projected to double; Singapore's to nearly triple from S$22 billion (2018) to S$59 billion by 2030 [1111Singapore Ministry of Health. Committee of Supply Debate 2024 — Healthcare statistics. Singapore: MOH; 2024.]. Demographic ageing is projected to reduce GDP growth by 0.3–1.2 percentage points per year by 2035, with Germany and Italy potentially recording growth below 1% [88Organisation for Economic Co-operation and Development (OECD). Fiscal sustainability and population ageing: OECD economic outlook. Paris: OECD Publishing; 2023.,1010International Monetary Fund (IMF). Fiscal monitor, April 2024. Washington (DC): IMF; 2024.], while the worker-to-retiree ratio falls from approximately four contributors per retiree today to fewer than two by 2030–2040 [1010International Monetary Fund (IMF). Fiscal monitor, April 2024. Washington (DC): IMF; 2024.,1212International Monetary Fund (IMF). Working paper WP/23/75: The economic impact of ageing populations. Washington (DC): IMF; 2023.]. These projections motivate this review's central question: whether Agentic AI can contribute meaningfully to moderating expenditure trajectories that no conventional policy instrument has yet resolved.
The projected range of 0.3–1.2 percentage points of annual GDP reduction by 2035 reflects country-specific estimates and should not be interpreted as a single aggregate trajectory. Germany and Italy sit at the higher end, while the United States sits at the lower [88Organisation for Economic Co-operation and Development (OECD). Fiscal sustainability and population ageing: OECD economic outlook. Paris: OECD Publishing; 2023.,1010International Monetary Fund (IMF). Fiscal monitor, April 2024. Washington (DC): IMF; 2024.].
The insufficiency of conventional responses
Governments have responded across four domains, including pension and labour-market reform, healthcare restructuring, workforce expansion, and digital health integration, yet each is facing binding constraints. Pension reform provides limited fiscal relief and often provokes political resistance, as recent protests in France illustrate [1313Vlandas T. The political economy of pension reform in France. J Eur Soc Policy. 2024;34(1):12–28.]. Preventive and community-based healthcare restructuring depends on the very workforce already under strain. Japan's long-term care insurance system and Singapore's Healthier SG programme both require a sustained labour supply to scale [66Kinsella K, Phillips DR. Global aging: the challenge of success. Popul Bull. 2005;60(1):1–40.,1414Singapore Ministry of Health. Healthier SG: Envisioning our healthcare system's next bound. Singapore: MOH; 2022.]. Workforce expansion through training and recruitment faces long lead times and retention challenges [77Ministry of Health, Labour and Welfare, Japan. Annual health, labour and welfare report 2023. Tokyo: MHLW; 2023.]. Digital health strategies, including Germany's DiGA programme, remain unevenly adopted and lack validated system-level impact [1414Singapore Ministry of Health. Healthier SG: Envisioning our healthcare system's next bound. Singapore: MOH; 2022.]. Consequently, even high-performing nations face pressures that existing policy instruments cannot fully resolve [1515AARP Public Policy Institute. Global aging readiness index 2024. Washington (DC): AARP; 2024.].
Agentic AI through a sociotechnical lens
This paper distinguishes three levels of healthcare AI. Narrow AI refers to single-task prediction or classification tools (e.g., diagnostic imaging models). Generative AI refers to large language models capable of natural language generation and reasoning across domains. Agentic AI (AAI) refers to systems that execute sustained, multi-step, goal-directed workflows across institutional boundaries, combining planning, memory, environmental interaction, and feedback under structured human oversight. The boundary between generative and agentic AI is functional rather than architecturally fixed and becomes increasingly fluid as persistent context and tool-use frameworks mature.
AAI offers potential capabilities that are conceptually aligned with the pressures facing ageing health systems. Unlike narrow clinical AI limited to prediction tasks, AAI integrates planning, memory, environmental interaction, and feedback to execute sustained workflows across institutional boundaries [1616Wang L. A survey on large language model-based autonomous agents. Front Comput Sci. 2024;18(6):1–26.]. For example, an AAI system could detect early clinical deterioration from home-monitoring data, initiate a telehealth consultation, and coordinate follow-up care under defined human oversight.
This review adopts sociotechnical systems theory, including the NASSS framework [1717Greenhalgh T. Beyond adoption: the NASSS framework. J Med Internet Res. 2017;19(11).], as its analytical anchor. Technological success depends not only on technical performance but also on alignment with organisational structures, governance arrangements, financing models, and human roles. Applied to eldercare, this perspective generates a testable proposition that deployment outcomes are determined primarily by institutional conditions rather than algorithmic capability.
It is important to note that, although the AAF 3.0 framework and roadmap presented in this paper are structured around agentic AI architectures, the reviewed evidence base encompasses broader AI applications in healthcare, including narrow diagnostic AI and general-purpose digital health tools. This reflects the limited number of studies explicitly evaluating agentic systems at scale within eldercare settings.
The analysis addresses three research questions:
− RQ1 (Capability): What is the current and near-term evidential basis for AAI across remote monitoring, assistive robotics, diagnostic support, medication adherence, and workflow automation, and how does evidence vary with intervention complexity?
− RQ2 (Implementation): Which regulatory, financial, organisational, and infrastructural factors determine whether AI capability translates into population-level benefit, and how do these vary across national contexts?
− RQ3 (Equity and Sustainability): Under what conditions can AI be adopted to avoid widening inequities and contribute to fiscal moderation, and which governance and evidence gaps prevent validation at scale?
The sociotechnical lens positions institutional alignment rather than technical optimism as the organising principle for the roadmap that follows.
This review contributes to the emerging literature on AI and ageing societies by integrating demographic economics, implementation science, and agentic AI architectures into a unified sociotechnical framework for health system transformation.
This study employed a structured narrative review (SNR) with systematic elements to synthesise heterogeneous evidence across demography, health economics, artificial intelligence, and policy. Meta-analysis was not feasible due to disciplinary diversity, outcome heterogeneity, and the inclusion of grey literature. Search and screening procedures followed PRISMA 2020 guidance. A structured review protocol was developed before data extraction, but was not formally registered with a prospective registry; the review should therefore be interpreted as PRISMA-informed rather than fully PRISMA-compliant.
Search strategy and source selection
Searches were conducted in PubMed, Scopus, Web of Science, and IEEE Xplore, supplemented by arXiv, medRxiv, and grey literature from the OECD, WHO, United Nations, European Commission, and national health ministries. Publications from January 2020 to December 2025 were prioritised, and earlier landmark studies were included where sources identified as foundational are marked with a [Foundational] notation. Search terms covered four domains, including population ageing, healthcare system pressure, artificial intelligence and agentic systems, and geographic scope. Representative search terms are provided in Appendix A.
Grey literature, including policy documents, national strategy reports, and institutional data from the OECD, WHO, United Nations, and national health ministries, was included because key demographic, fiscal, and health system planning data relevant to this review are not routinely available in peer-reviewed journals. Preprints from arXiv and medRxiv were also included, where findings demonstrated methodological transparency and represented later-stage or widely cited work in the field. All grey literature was evaluated for data transparency, institutional credibility, and methodological clarity using the CASP adapted framework described below.
Screening and selection process
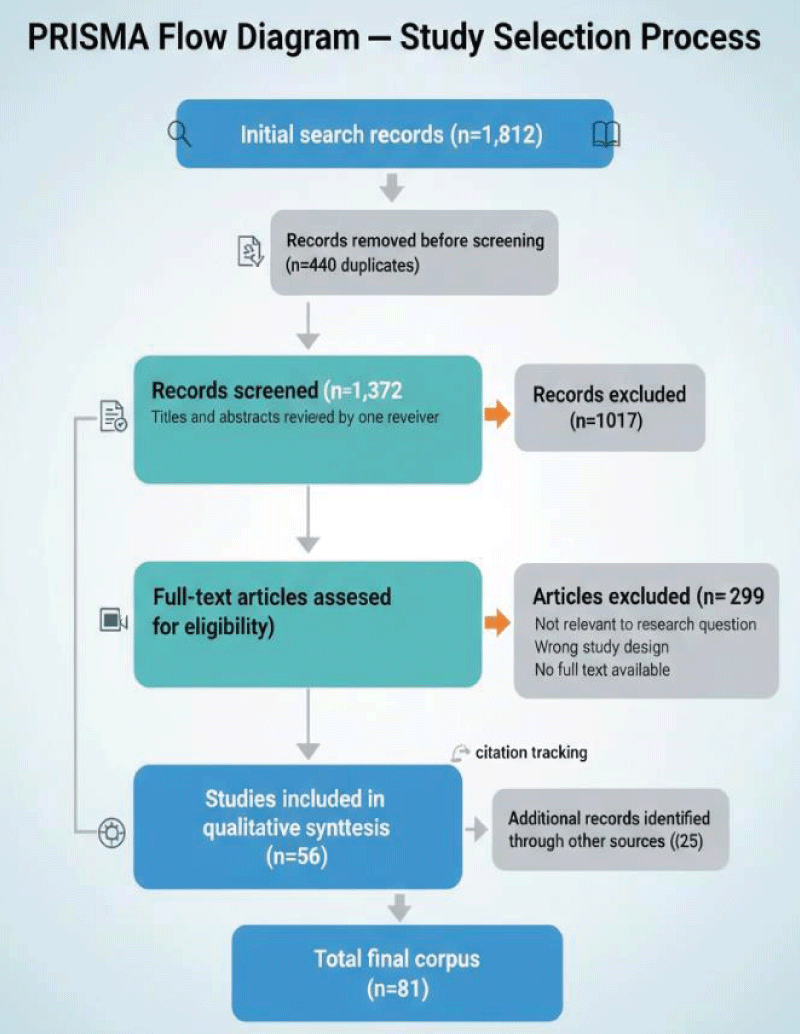
The search yielded 1,812 records, of which 440 duplicates were removed. Two reviewers independently screened 1,372 titles and abstracts, achieving strong inter-rater agreement (Cohen's κ = 0.81). Of the 355 full-text articles assessed, 56 met the inclusion criteria. An additional 25 sources identified through citation tracking resulted in a final sample of 81 included sources. The PRISMA flow diagram is presented in Figure 1.
Figure 1: PRISMA Flow Diagram — Study Selection Process.
Inclusion required relevance to population ageing or artificial intelligence in healthcare within OECD contexts, together with empirical evidence or methodologically transparent institutional data. Opinion pieces, non-healthcare AI studies, and commercial market research were excluded. Disagreements between reviewers were resolved through consensus.
Quality appraisal, data extraction, and synthesis
Empirical studies were appraised using an adapted CASP framework assessing methodological rigour, relevance, outcome validity, follow-up adequacy, and reporting transparency. Systematic reviews were evaluated using AMSTAR-2 criteria, and institutional grey literature was assessed for data transparency and methodological clarity. Narrative synthesis followed a framework synthesis approach anchored to the NASSS framework [1717Greenhalgh T. Beyond adoption: the NASSS framework. J Med Internet Res. 2017;19(11).] with thematic mapping of evidence against the six NASSS domains (condition, technology, value proposition, adopter system, organisation, and wider system). This approach was selected over thematic or realist synthesis because the NASSS framework provides an established theoretical architecture directly applicable to complex health technology adoption — the central analytical task of this review.
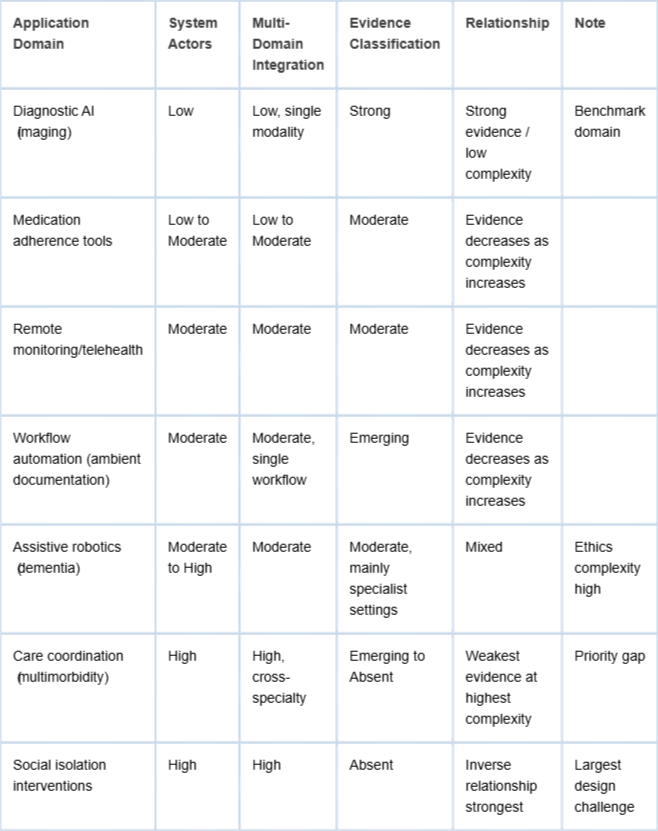
Intervention complexity was assessed along two dimensions: the number of system actors involved (e.g., patients, clinicians, administrators, and institutional systems) and the degree of multi-domain integration required for deployment. These dimensions were derived inductively from the literature and informed the classification presented in Table 2. Evidence strength was operationalised using pre specified criteria applied independently by both reviewers with consensus resolution (Appendix Table B2): “Strong” required at least two systematic reviews or meta analyses with low risk of bias; “Moderate” required at least two RCTs or well-designed prospective cohort studies with consistent findings; “Emerging” required at least one controlled study or consistent observational evidence across two or more settings; and “Absent” referred to evidence limited to expert opinion or the absence of peer reviewed studies identified in the search.
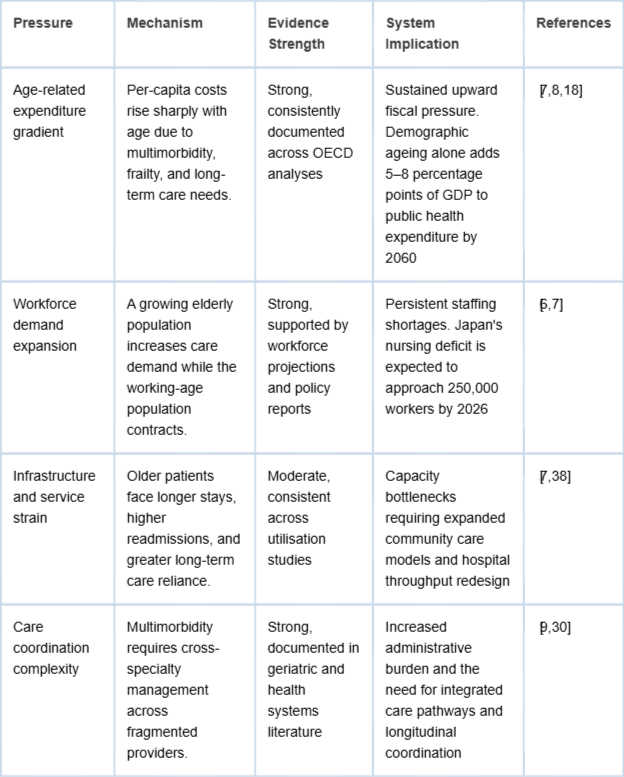
Table 1: Structural Pressures of Population Ageing on Healthcare Systems.
Table 2: Inverse Evidence: Complexity Relationship Across AI Application Domains.
Evidence strength was assigned at the domain level using pre-specified operational criteria applied independently by both reviewers with consensus resolution. The full classification framework is presented in Appendix Table B2.
Evidence synthesis: Structural pressures, AI applications, and institutional constraint
Structural pressures on ageing health systems
Population ageing generates healthcare strain through three compounding mechanisms, including rising age-related expenditure, workforce contraction, and increasing care complexity. Per-capita costs for those aged 65 and above are several times higher than for working-age populations and rise sharply beyond age 80. OECD and European Commission projections indicate that ageing alone will add several percentage points to GDP and public health expenditure across member states [88Organisation for Economic Co-operation and Development (OECD). Fiscal sustainability and population ageing: OECD economic outlook. Paris: OECD Publishing; 2023.,1818European Commission. The 2024 ageing report: Economic and budgetary projections for EU member states. Luxembourg: Publications Office of the European Union; 2024.]. Growth is concentrated among those aged 75 and above, the highest utilisation subgroup, and old-age dependency ratios in the most affected nations are projected to approach one older adult per working-age individual later this century [11United Nations, Department of Economic and Social Affairs, Population Division. World population prospects 2024. New York: United Nations; 2024.]. Multimorbidity further compounds strain because most adults over 65 live with two or more chronic conditions requiring cross-specialty coordination [99Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, Brayne C, Burns A, Cohen-Mansfield J, Cooper C, Costafreda SG, Dias A, Fox N, Gitlin LN, Howard R, Kales HC, Kivimäki M, Larson EB, Ogunniyi A, Orgeta V, Ritchie K, Rockwood K, Sampson EL, Samus Q, Schneider LS, Selbæk G, Teri L, Mukadam N. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020 Aug 8;396(10248):413-446. doi: 10.1016/S0140-6736(20)30367-6. Epub 2020 Jul 30. Erratum in: Lancet. 2023 Sep 30;402(10408):1132. doi: 10.1016/S0140-6736(23)02043-3. PMID: 32738937; PMCID: PMC7392084.]. Table 1 summarises these pressures. Note: France appears throughout this review as a comparative reference economy and in the cross-country data presented in Appendix E. It is not included as a primary case in the Section 3 synthesis tables, as its demographic and fiscal profile places it in an intermediate category relative to the seven economies where the evidence base is most developed.
The four pressures in Table 1 are mutually reinforcing: age-related expenditure growth partly reflects care coordination complexity, while workforce demand is intensified by institutional fragmentation. Evidence is strongest in expenditure and care coordination, indicating these are established system-level realities requiring immediate policy attention.
Two cross-cutting patterns shape the remainder of the analysis. Evidence strength is inversely related to intervention complexity. The multi-domain applications most needed in ageing health systems, therefore, have the weakest evidence base, reflecting underinvestment in complex interventions. Implementation of context also matters more than technical performance. Factors such as workflow integration, clinician training, institutional readiness, and digital literacy influence outcomes more than algorithm accuracy [1717Greenhalgh T. Beyond adoption: the NASSS framework. J Med Internet Res. 2017;19(11).,1919Cresswell K. NHS Scotland's decision support platform: a formative qualitative evaluation. BMJ Health Care Inform. 2020;27(1):e100033.]. Table 2 illustrates this inverse relationship across AI domains. Detailed cross-country demographic and fiscal projections for major ageing economies are provided in Appendix E (Tables E1–E2) to reduce table density in the main manuscript.
The inverse evidence–complexity pattern in Table 2 represents a key finding for research prioritisation: AI domains most capable of addressing systemic eldercare pressures, particularly care coordination and social isolation, lack validated evidence, while the strongest evidence base (diagnostic imaging AI) addresses only a narrow aspect of geriatric care complexity. This gap informs the research agenda in Section 4.6 and the phased roadmap in Section 4.4.
Three patterns from the cross-country demographic and fiscal projections in Appendix E (Tables E1–E2) are particularly important. South Korea and Singapore face the most severe projected dependency ratios by 2050, at 79.0 and 85.0, respectively, but their fiscal preparedness differs sharply. Singapore’s CPF compulsory savings model keeps ageing-related spending near 10% of GDP, compared with about 16 percent in South Korea. Italy and France already spend about 28% - 30% of GDP on ageing-related programmes, leaving limited fiscal space for new technology investments. The United States faces lower structural pressure because of a relatively younger population and an immigration-supported workforce, despite having the highest per-capita health spending. These differences shape AI deployment sequencing. Countries with stronger fiscal capacity and high digital readiness, including Singapore, Germany, and South Korea, are better positioned for early Phase 2 pilots, while countries with higher fiscal risk, including Italy and France, may require fiscal consolidation before large-scale deployment. Appendix E presents detailed demographic and fiscal projections across ageing economies.
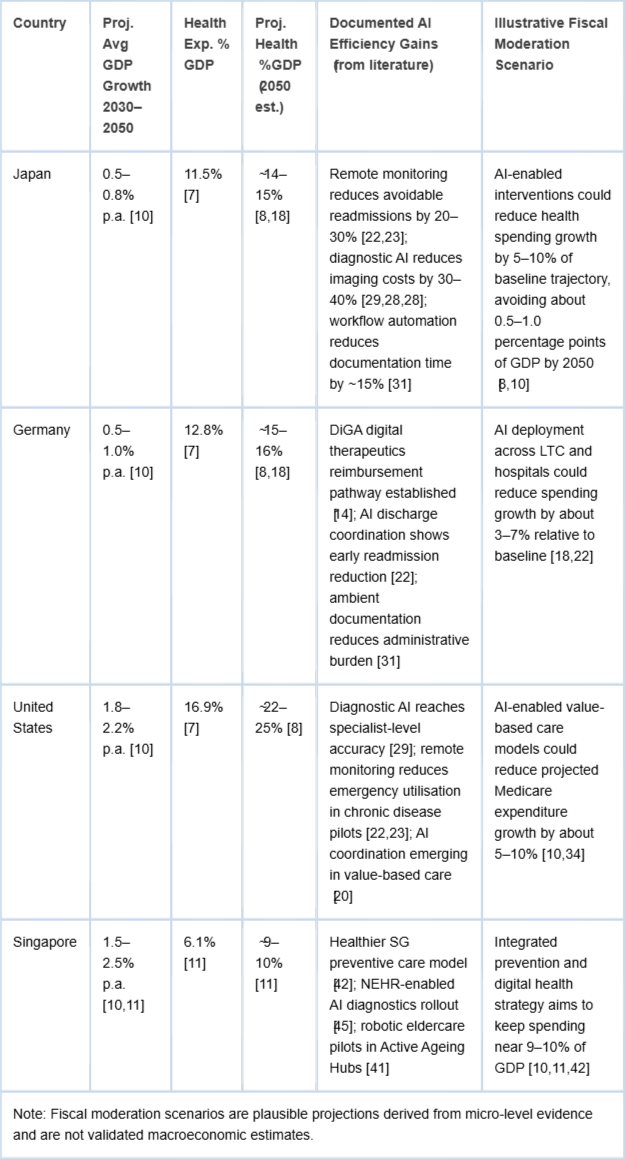
Table 3 shows a consistent divergence between projected GDP growth and healthcare expenditure: economies with the lowest growth, particularly Japan and Germany, face the steepest increases in health spending, creating compounding fiscal constraints. The fiscal moderation scenarios in the final column are illustrative hypotheses based on micro-level evidence, not validated macroeconomic projections.
Table 3: GDP Growth vs. Healthcare Expenditure Pressure in Selected Ageing Economies.
AI applications in ageing health systems
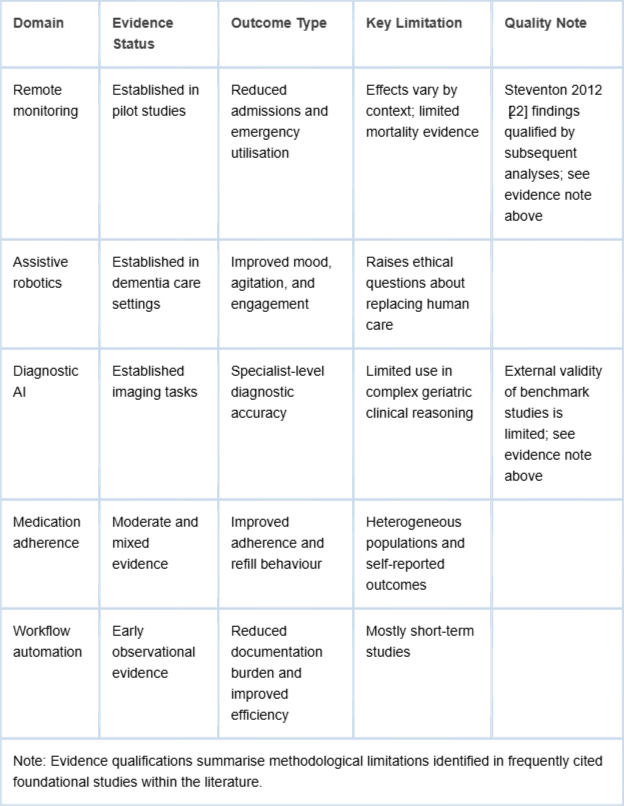
Across five principal domains, a consistent pattern emerges. AI tools are most effective when used to support structured care pathways rather than replace human judgment [2020Matheny ME, Whicher D, Thadaney Israni S. Artificial Intelligence in Health Care: A Report From the National Academy of Medicine. JAMA. 2020 Feb 11;323(6):509-510. doi: 10.1001/jama.2019.21579. PMID: 31845963.,2121Kelly CJ. Key challenges for delivering clinical impact with artificial intelligence. Nat Med. 2019;25(1):44–56.]. Evidence for foundational applications such as remote monitoring and socially assistive robotics is largely based on trials conducted before 2018. Later studies, including systematic reviews published between 2020 and 2024, broadly replicate the directional findings of earlier work, though they do not extend follow-up duration or population scale sufficiently to resolve questions about long-term cost-effectiveness [2020Matheny ME, Whicher D, Thadaney Israni S. Artificial Intelligence in Health Care: A Report From the National Academy of Medicine. JAMA. 2020 Feb 11;323(6):509-510. doi: 10.1001/jama.2019.21579. PMID: 31845963.-2525Moyle W. Exploring the effect of companion robots on emotional expression in older adults with dementia. J Gerontol Nurs. 2017;43(5):27–35.]. This pattern suggests continued underinvestment in complex intervention research and highlights the research gaps discussed in Section 4.6. Key methodological limitations and qualifications associated with widely cited studies are summarised in Table 4.
Table 4: Evidence and Limitations of AI Applications in Ageing Health Systems.
Remote monitoring systems are associated with reduced hospital admissions and emergency utilisation among chronic disease populations [2222Steventon A, Bardsley M, Billings J, Dixon J, Doll H, Hirani S, Cartwright M, Rixon L, Knapp M, Henderson C, Rogers A, Fitzpatrick R, Hendy J, Newman S; Whole System Demonstrator Evaluation Team. Effect of telehealth on use of secondary care and mortality: findings from the Whole System Demonstrator cluster randomised trial. BMJ. 2012 Jun 21;344:e3874. doi: 10.1136/bmj.e3874. PMID: 22723612; PMCID: PMC3381047.,2323Klersy C, De Silvestri A, Gabutti G, Regoli F, Auricchio A. A meta-analysis of remote monitoring of heart failure patients. J Am Coll Cardiol. 2009 Oct 27;54(18):1683-94. doi: 10.1016/j.jacc.2009.08.017. Erratum in: J Am Coll Cardiol. 2010 May 11;55(19):2185. PMID: 19850208.]. However, results depend on context, and evidence for mortality reduction or delayed institutionalisation remains limited. Socially assistive robots improve agitation, mood, and engagement in dementia care [2424Wada K. Robot therapy for dementia patients. Proc World Acad Sci Eng Technol. 2008;31:543–548.-2626Moyle W, Jones CJ, Murfield JE, Thalib L, Beattie ERA, Shum DKH, O'Dwyer ST, Mervin MC, Draper BM. Use of a Robotic Seal as a Therapeutic Tool to Improve Dementia Symptoms: A Cluster-Randomized Controlled Trial. J Am Med Dir Assoc. 2017 Sep 1;18(9):766-773. doi: 10.1016/j.jamda.2017.03.018. Epub 2017 Aug 2. PMID: 28780395.]. Their use also raises governance questions about augmentation versus substitution of human care. Diagnostic AI achieves specialist-level accuracy in imaging tasks [2727Esteva A, Kuprel B, Novoa RA, Ko J, Swetter SM, Blau HM, Thrun S. Dermatologist-level classification of skin cancer with deep neural networks. Nature. 2017 Feb 2;542(7639):115-118. doi: 10.1038/nature21056. Epub 2017 Jan 25. Erratum in: Nature. 2017 Jun 28;546(7660):686. doi: 10.1038/nature22985. PMID: 28117445; PMCID: PMC8382232.-2929Liu X. A comparison of deep learning performance against healthcare professionals. Nat Med. 2019;25(6):1009–1015.]. However, it does not generalise well to complex geriatric clinical decision-making. Medication adherence tools show modest and mixed improvements [3030Rajpurkar P, Chen E, Banerjee O, Topol EJ. AI in health and medicine. Nat Med. 2022 Jan;28(1):31-38. doi: 10.1038/s41591-021-01614-0. Epub 2022 Jan 20. PMID: 35058619.]. Ambient documentation systems show early evidence of reduced clinician administrative burden, although studies remain short-term and observational [3131Sinsky CA. Metrics for assessing physician activity using electronic health records: the Association of American Medical Colleges approach. J Am Med Inform Assoc. 2021;28(4):840–847.].
The evidence patterns in Table 4 indicate that even well-established AI application domains have limitations for population-level eldercare: remote monitoring outcomes vary by care context, and diagnostic AI has not consistently performed well in complex, multi-morbid geriatric cases. These constraints underscore the need for structured pilot validation, as outlined in Phase 2 of the roadmap, before large-scale deployment.
Economic evidence: Microeconomic gains and macroeconomic uncertainty
Economic evidence is limited by the absence of a validated macroeconomic evaluation. The central question is whether AI can meaningfully moderate demographic expenditure growth at the population scale. This question remains unanswered in the peer-reviewed literature. The IMF Fiscal Monitor (2024) projects that public health spending will rise by 2.0–3.5 percentage points of GDP by 2050 under baseline scenarios and by 3.5–6.0 points under adverse trajectories [1010International Monetary Fund (IMF). Fiscal monitor, April 2024. Washington (DC): IMF; 2024.]. Claims that AI could moderate these trends should therefore be treated as hypotheses until longitudinal evidence emerges.
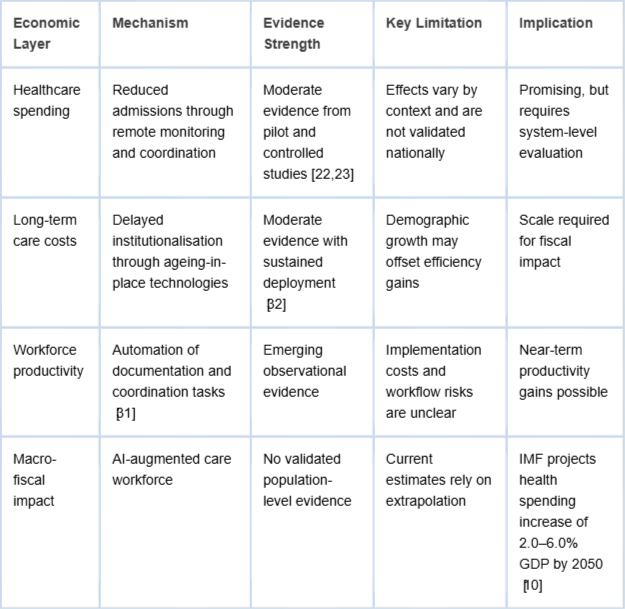
At the microeconomic level, studies report incremental savings from reduced admissions through remote monitoring and care coordination [2222Steventon A, Bardsley M, Billings J, Dixon J, Doll H, Hirani S, Cartwright M, Rixon L, Knapp M, Henderson C, Rogers A, Fitzpatrick R, Hendy J, Newman S; Whole System Demonstrator Evaluation Team. Effect of telehealth on use of secondary care and mortality: findings from the Whole System Demonstrator cluster randomised trial. BMJ. 2012 Jun 21;344:e3874. doi: 10.1136/bmj.e3874. PMID: 22723612; PMCID: PMC3381047.,2323Klersy C, De Silvestri A, Gabutti G, Regoli F, Auricchio A. A meta-analysis of remote monitoring of heart failure patients. J Am Coll Cardiol. 2009 Oct 27;54(18):1683-94. doi: 10.1016/j.jacc.2009.08.017. Erratum in: J Am Coll Cardiol. 2010 May 11;55(19):2185. PMID: 19850208.]. Some studies report long-term care gains from delayed institutionalization [3232Organisation for Economic Co-operation and Development (OECD). The economic benefit of promoting healthy ageing and community care. Paris: OECD Publishing; 2025.]. Emerging evidence also suggests productivity gains from documentation automation [3131Sinsky CA. Metrics for assessing physician activity using electronic health records: the Association of American Medical Colleges approach. J Am Med Inform Assoc. 2021;28(4):840–847.]. Cost-effectiveness findings differ across financing models. In Japan’s publicly funded system, savings from avoided institutionalisation align incentives. In Germany’s Bismarckian model, reimbursement reform across statutory funds is required. In Singapore’s Medisave-based system, central governance may accelerate implementation, but equity risks remain. The economic case for AI in eldercare is therefore system-specific and cannot be derived from aggregate evidence without considering financing models, incentives, and population baseline.
Table 5 indicates that the economic case for AI in eldercare is strongest at the microeconomic level, where pilot evidence shows incremental savings from reduced admissions and delayed institutionalisation, while macro fiscal impact lacks validated population-level evidence. This asymmetry between micro-level signals and macro fiscal uncertainty represents the key evidentiary gap addressed by the longitudinal research agenda in Section 4.6.
Table 5: Economic Evidence on AI in Ageing Health Systems.
Governance, regulation, and the algorithmic bias problem
Under the EU AI Act (2024), AI systems that qualify as medical devices, including diagnostic, clinical decision support, or patient management tools, are classified as high risk. This classification requires conformity assessment, human oversight, transparency, data governance, and post-market monitoring [3333European Commission. Regulation laying down harmonised rules on artificial intelligence (EU AI Act). Brussels: European Commission; 2024.]. Agentic eldercare systems that execute multi-step clinical workflows fall within this category, so compliance timelines must be integrated into implementation planning from the beginning. Japan, Singapore, and South Korea face similar governance challenges but lack the EU’s coordinated regulatory structure. The OECD has also identified responsible AI deployment in healthcare as a policy priority [3434Organisation for Economic Co-operation and Development (OECD). AI in health: Action plan for responsible deployment. Paris: OECD; 2024.]. Large language models introduce additional risks because they can generate clinically plausible but incorrect outputs. This reinforces the need for human oversight at critical clinical decision points [3535Meskó B, Topol EJ. The imperative for regulatory oversight of large language models (or generative AI) in healthcare. NPJ Digit Med. 2023 Jul 6;6(1):120. doi: 10.1038/s41746-023-00873-0. PMID: 37414860; PMCID: PMC10326069.].
Algorithmic bias represents another institutional constraint. Obermeyer et al. demonstrated systematic racial bias in a US risk scoring algorithm [3636Obermeyer Z, Powers B, Vogeli C, Mullainathan S. Dissecting racial bias in an algorithm used to manage the health of populations. Science. 2019 Oct 25;366(6464):447-453. doi: 10.1126/science.aax2342. PMID: 31649194.]. Subsequent studies in Nordic and UK systems identify similar risks linked to the underrepresentation of rural, minority, and oldest old populations [3737Organisation for Economic Co-operation and Development (OECD), European Commission. Health at a glance: Europe 2024. Paris: OECD Publishing; 2024.]. Bias patterns are context-specific. East Asian datasets may appear ethnically homogeneous but can still underrepresent socioeconomically marginalised elderly groups. Auditing must therefore rely on locally representative data. In geriatric care, this issue is particularly important because underrepresented populations often have the highest care needs and the least alternative access to services.
Equity as a structural barrier, not an afterthought
Equity implications extend beyond algorithmic bias to structural determinants shaping whether deployment narrows or widens disparities. Three inequality axes are central. Urban-rural divides show rural older adults face weaker digital infrastructure and higher illiteracy, with remote monitoring uptake consistently lower in rural settings [3030Rajpurkar P, Chen E, Banerjee O, Topol EJ. AI in health and medicine. Nat Med. 2022 Jan;28(1):31-38. doi: 10.1038/s41591-021-01614-0. Epub 2022 Jan 20. PMID: 35058619.,3838Organisation for Economic Co-operation and Development (OECD). Adapting health systems to an ageing population. Paris: OECD Publishing; 2024.], meaning those most isolated from conventional care are least likely to benefit from AI alternatives. Digital literacy gradients show telehealth utilisation among adults aged 75 and above remains substantially lower than among younger cohorts across OECD nations [3030Rajpurkar P, Chen E, Banerjee O, Topol EJ. AI in health and medicine. Nat Med. 2022 Jan;28(1):31-38. doi: 10.1038/s41591-021-01614-0. Epub 2022 Jan 20. PMID: 35058619.,3737Organisation for Economic Co-operation and Development (OECD), European Commission. Health at a glance: Europe 2024. Paris: OECD Publishing; 2024.], risking exclusion of the oldest old with the highest care needs. Socioeconomic stratification shows out of pocket costs for assistive technologies concentrate quality gains among already advantaged populations [3636Obermeyer Z, Powers B, Vogeli C, Mullainathan S. Dissecting racial bias in an algorithm used to manage the health of populations. Science. 2019 Oct 25;366(6464):447-453. doi: 10.1126/science.aax2342. PMID: 31649194.,3737Organisation for Economic Co-operation and Development (OECD), European Commission. Health at a glance: Europe 2024. Paris: OECD Publishing; 2024.]. Equity must shape deployment sequencing, prioritising underserved groups in pilot design rather than treating them as post deployment audit categories.
Comparative institutional readiness
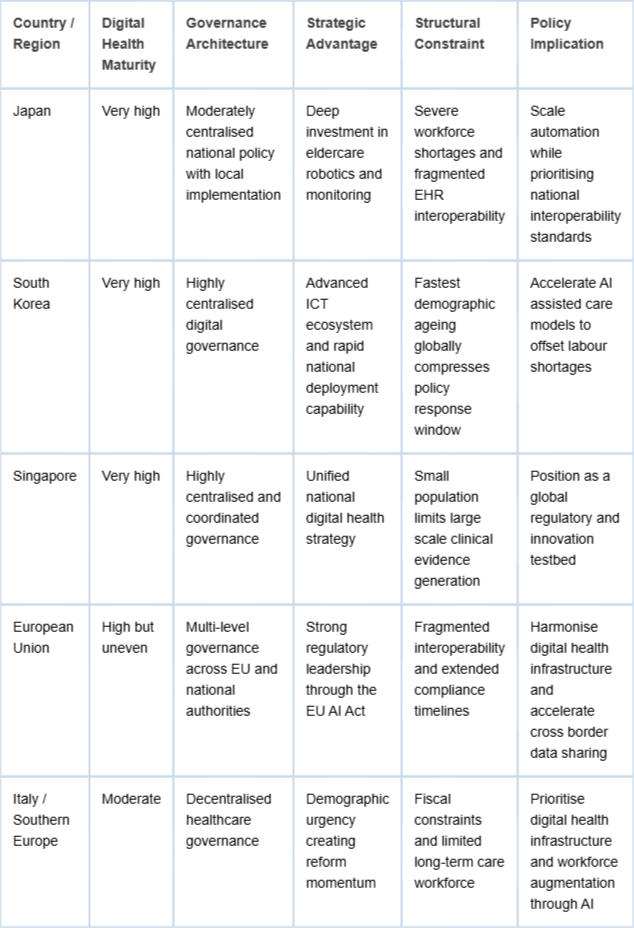
Institutional readiness patterns reinforce the sociotechnical thesis that adoption trajectories are shaped as strongly by governance design, infrastructure maturity, and public trust as by technical capability. Japan combines acute demographic urgency with sustained robotics investment but faces workforce shortages and fragmented EHR systems [66Kinsella K, Phillips DR. Global aging: the challenge of success. Popul Bull. 2005;60(1):1–40.]. South Korea benefits from an advanced digital infrastructure, yet it confronts the fastest demographic transition globally, which compresses the implementation window [22Organisation for Economic Co-operation and Development (OECD). Health at a glance 2023: OECD indicators. Paris: OECD Publishing; 2023. doi:10.1787/7a7afb35-en,3939Statistics Korea. Population projections for Korea. Seoul: Statistics Korea; 2023.]. Singapore's centralised governance enables rapid digital health coordination, though its small population limits evidence generalization [1414Singapore Ministry of Health. Healthier SG: Envisioning our healthcare system's next bound. Singapore: MOH; 2022.,4040Singapore Ministry of Health. Action plan for successful ageing. Singapore: MOH; 2023.]. Germany and Nordic states lead EU digital health adoption, and the EU AI Act's uniform high-risk classification extends regulatory timelines across member states [3333European Commission. Regulation laying down harmonised rules on artificial intelligence (EU AI Act). Brussels: European Commission; 2024.].
A consistent pattern emerges because demographic urgency often diverges from institutional readiness. Italy and Southern Europe face sharp ageing pressures alongside constrained fiscal and digital capacity. Japan's technological leadership coexists with workforce and interoperability constraints. These governance mismatches, rather than technical limitations, define the central challenge for the roadmap that follows.
Singapore as a governance first benchmark for ageing system transformation
Singapore provides one of the clearest examples of governance-aligned preparation for population ageing. The country faces one of the steepest projected dependency ratios globally, with the old age dependency ratio expected to rise from 24.2 in 2023 to approximately 85 by 2050. At the same time, national healthcare expenditure is projected to reach about S$59 billion by 2030. In response, the government has implemented a coordinated national strategy that integrates prevention, financing, workforce policy, digital infrastructure, and cross-sector governance [1111Singapore Ministry of Health. Committee of Supply Debate 2024 — Healthcare statistics. Singapore: MOH; 2024.,4141Ministerial Committee on Ageing. Action plan for successful ageing 2023 update. Singapore: MCA; 2023.].
Preventive system transformation – The healthier SG
The Healthier SG initiative, launched in 2022, restructures primary care around longitudinal preventive management. All residents aged 40 and above are enrolled with a designated primary care physician and receive personalised preventive plans supported by digital monitoring tools, including the Healthy 365 application. The government has committed about S$1 billion over five years to support this preventive shift, which aims to reduce costly hospital utilisation before the demographic peak [4242Ministry of Health Singapore (MOH). Healthier SG white paper 2022. Singapore: MOH; 2022.].
Financing architecture – The ‘3M’ framework
Singapore's financing structure combines three complementary mechanisms. Medisave provides mandatory individual health savings contributions of roughly 8 to 10.5 percent of income. MediShield Life provides universal catastrophic insurance coverage. MediFund operates as a public safety net for patients unable to meet residual costs. This layered design distributes responsibility across individuals’ insurance pools and the government while containing fiscal risk and limiting moral hazard [4343Ministry of Health Singapore (MOH). Healthcare financing white paper 2023. Singapore: MOH; 2023.].
To mitigate labour shortages associated with ageing, the government has progressively extended workforce participation. The statutory retirement age has been raised to 63, with a planned increase to 65 by 2030, while the re-employment age will rise to 70. Labour force participation among adults aged 65 to 69 increased from 31.4 percent in 2013 to 43.3 percent in 2023 which demonstrates that policy incentives and regulatory reform can significantly extend productive ageing [4444Ministry of Manpower Singapore (MOM). Labour force in Singapore 2023. Singapore: MOM; 2023.].
Digital health infrastructure
Singapore has established national digital health infrastructure through the National Electronic Health Record system which integrates clinical data across the healthcare system. The Digital Health Blueprint supports nationwide interoperability and data governance. AI enabled diagnostic tools for conditions such as diabetic retinopathy and stroke detection are being deployed while robotic assistants have been piloted in community and long-term care environments. These systems collectively represent operational foundations for the Integrated Perception pillar of the AAF 3.0 framework [4545Integrated Health Information Systems (IHiS). Digital health blueprint 2023. Singapore: IHiS; 2023.].
Whole of government governance – APSA 2023
The Action Plan for Successful Ageing coordinates more than 200 initiatives across health housing, employment, transport and community participation. Active Ageing Centers operate nationwide to support community engagement and care coordination. The Seniors Go Digital initiative has trained more than 200000 older adults in digital literacy which directly addresses digital exclusion risks associated with technology-based healthcare delivery [4141Ministerial Committee on Ageing. Action plan for successful ageing 2023 update. Singapore: MCA; 2023.].
Implications for comparative policy
Singapore institutional model is not directly transferable because its city state scale centralised governance and fiscal reserves create enabling conditions that larger federated systems do not possess. Nevertheless, the sequencing of reforms provides a clear policy lesson. Preventive care financing digital infrastructure and cross sector governance were established before demographic pressures reached their peak. In contrast many ageing economies attempt to deploy technological solutions after fiscal and workforce pressures have already intensified.
From a NASSS perspective Singapore demonstrates favourable conditions across all six domains including technology readiness value proposition adopter acceptance organisational embedding and system level governance. For larger ageing economies including Japan South Korea Germany and Italy the principal barrier to AI enabled healthcare adoption therefore lies less in algorithmic capability and more in institutional alignment.
Table 6 reinforces this finding by showing that countries with the highest demographic urgency, including Japan, South Korea, and Singapore, also exhibit high digital health maturity but face distinct structural constraints, from workforce shortages in Japan to compressed policy timelines in South Korea. Across contexts, institutional readiness, rather than technical capability, emerges as the primary constraint on AI enabled healthcare deployment for ageing populations.
Table 6: Comparative Institutional Readiness for AI-Enabled Healthcare in Ageing Societies.
Discussion and policy implications for AI implementation in ageing health systems
The central institutional thesis
The synthesis across Sections 3.1 to 3.6 supports a consistent conclusion. Where AI underperforms relative to technical potential, four institutional factors limit impact more reliably than model performance: fragmented data architectures, misaligned incentives, regulatory uncertainty, and exclusionary deployment design. In ageing systems, institutional fragility amplifies technological limitations [1717Greenhalgh T. Beyond adoption: the NASSS framework. J Med Internet Res. 2017;19(11).,2121Kelly CJ. Key challenges for delivering clinical impact with artificial intelligence. Nat Med. 2019;25(1):44–56.].
The NASSS framework maps directly onto observed constraints including condition complexity linked to multimorbidity technology complexity from cross domain orchestration uncertain value propositions without macroeconomic validation adopter resistance interoperability limits and regulatory and financing structures that mediate translation from effectiveness to system utility [1717Greenhalgh T. Beyond adoption: the NASSS framework. J Med Internet Res. 2017;19(11).]. A further tension concerns relational care quality. Evidence from socially assistive robotics shows that measured improvements in agitation or mood do not determine whether care is enhanced or diminished. Outcomes depend on governance decisions regarding augmentation versus substitution [2424Wada K. Robot therapy for dementia patients. Proc World Acad Sci Eng Technol. 2008;31:543–548.-2626Moyle W, Jones CJ, Murfield JE, Thalib L, Beattie ERA, Shum DKH, O'Dwyer ST, Mervin MC, Draper BM. Use of a Robotic Seal as a Therapeutic Tool to Improve Dementia Symptoms: A Cluster-Randomized Controlled Trial. J Am Med Dir Assoc. 2017 Sep 1;18(9):766-773. doi: 10.1016/j.jamda.2017.03.018. Epub 2017 Aug 2. PMID: 28780395.]. Technological capability is therefore necessary but insufficient. Population level benefits depend on institutional alignment and capability without governance produces pilots that cannot scale.
The agentic AI framework (AAF 3.0): Derivation and differentiation
The AAF 3.0 is more precisely described as an agentic AI domain-mapping matrix, a conceptual applied implementation tool derived deductively from the structural pressures identified in Section 3.1 and positioned as an extension of the NASSS framework specifically for agentic AI architectures. The designation “3.0” reflects a conceptual progression in healthcare AI capability from narrow clinical AI (primarily diagnostic and single-task predictive systems) to generative AI (multi-domain language reasoning) and finally to agentic AI (sustained multi-step workflow orchestration with environmental feedback). This versioning is original to this paper and should be understood as a descriptive periodisation of evolving AI capability in healthcare contexts rather than a reference to a previously established framework lineage; no AAF 1.0 or 2.0 frameworks exist in prior literature.
AAF 3.0 differs from NASSS in scope and purpose. NASSS is a general-purpose implementation framework applicable to any complex health technology. AAF 3.0 uses the NASSS analytical structure as its foundation but organises it around the specific functional capabilities of agentic AI systems — each derived from a distinct structural pressure. Where NASSS asks 'which implementation factors matter?', AAF 3.0 asks 'which agentic capabilities potentially address which system pressures, at what evidence stage, and under what governance conditions?'. This applied specificity is its contribution.
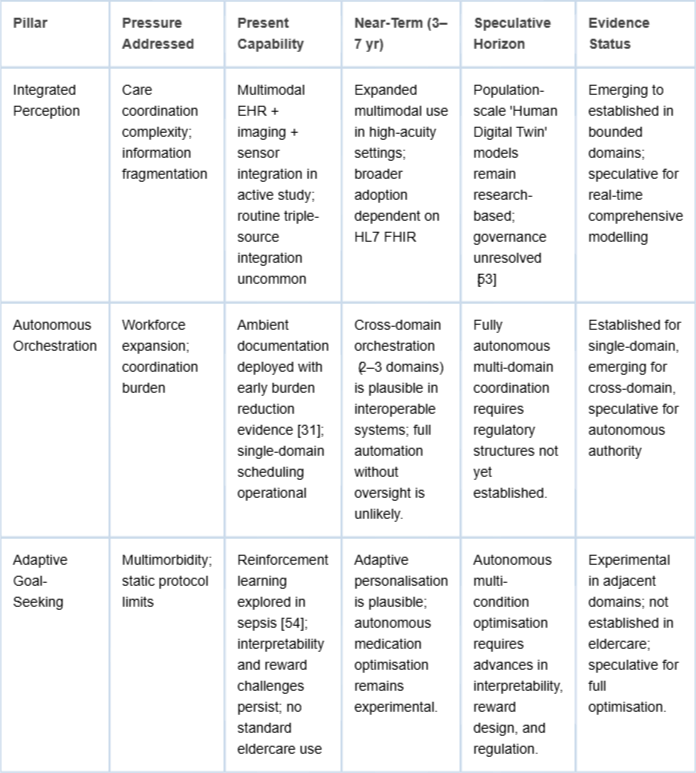
Each pillar is designed to correspond to a system constraint: Integrated Perception addresses information fragmentation; Autonomous Orchestration may augment coordination capacity under workforce contraction; Adaptive Goal-Seeking is conceptually positioned to respond to multimorbidity beyond static single-disease protocols. Systems are characterised as agentic when they execute sustained multi-step, cross-system workflows toward defined care objectives under structured human oversight.
Table 7 indicates a consistent temporal gradient. Integrated Perception is most developed in bounded domains but constrained by interoperability gaps. Autonomous Orchestration shows the strongest near-term trajectory in single domain automation. Adaptive Goal Seeking remains the most experimentally distant. Near term implementation should potentially prioritise Perception and bounded Orchestration while treating Adaptive Goal Seeking as a medium-term research investment.
Operational bottlenecks and AI entry points in ageing health systems
Three potentially high-impact, deployment-ready targets are identified. These form the operational context for the phased roadmap that follows in Section 4.4. (1) Documentation burden in geriatric and community care is the most defensible initial target, combining a well-documented inefficiency with commercially available solutions and relatively contained workflow redesign [3131Sinsky CA. Metrics for assessing physician activity using electronic health records: the Association of American Medical Colleges approach. J Am Med Inform Assoc. 2021;28(4):840–847.]. (2) Discharge coordination and readmission prevention for multimorbid older adults form the second priority [2222Steventon A, Bardsley M, Billings J, Dixon J, Doll H, Hirani S, Cartwright M, Rixon L, Knapp M, Henderson C, Rogers A, Fitzpatrick R, Hendy J, Newman S; Whole System Demonstrator Evaluation Team. Effect of telehealth on use of secondary care and mortality: findings from the Whole System Demonstrator cluster randomised trial. BMJ. 2012 Jun 21;344:e3874. doi: 10.1136/bmj.e3874. PMID: 22723612; PMCID: PMC3381047.,2323Klersy C, De Silvestri A, Gabutti G, Regoli F, Auricchio A. A meta-analysis of remote monitoring of heart failure patients. J Am Coll Cardiol. 2009 Oct 27;54(18):1683-94. doi: 10.1016/j.jacc.2009.08.017. Erratum in: J Am Coll Cardiol. 2010 May 11;55(19):2185. PMID: 19850208.]. (3) Early deterioration detection through remote monitoring represents a third entry point, targeting high-cost acute events. All three targets share a critical property: they permit structured workflow redesign before AI deployment, reducing reliance on technological substitution.
A sociotechnical phased roadmap
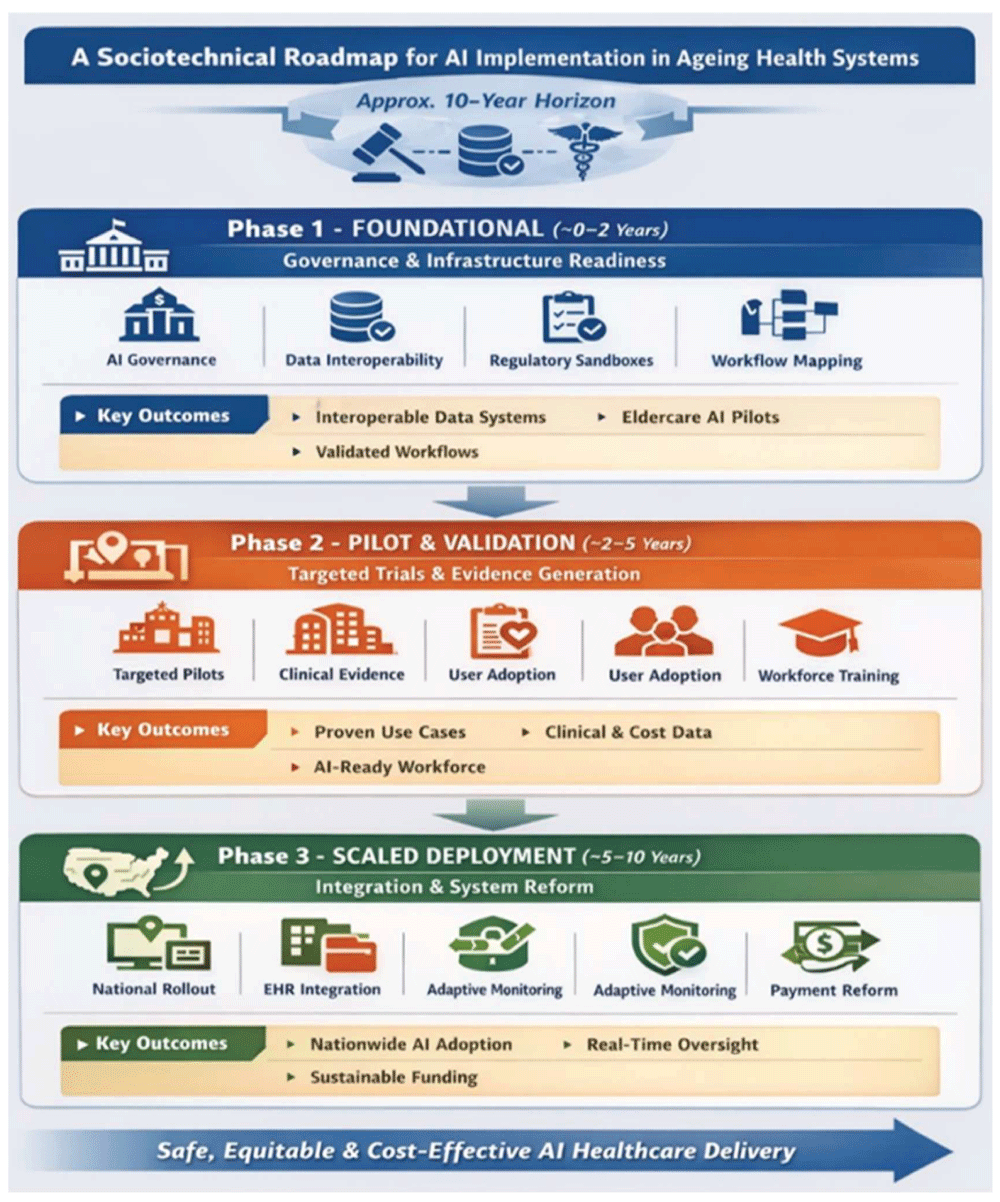
The roadmap translates the institutional thesis into a governance sequenced implementation strategy across a ten-year horizon. Phase durations are indicative and draw on observed timelines for large-scale digital health reform regulatory pathway development cycles for high-risk adaptive technologies and implementation science evidence on pilot to scale transitions. Higher readiness systems may progress at the lower end of these ranges, while lower readiness contexts should anticipate longer timelines (Figure 2).
Figure 2: A Sociotechnical Roadmap for AI Implementation in Ageing Health Systems.
Phase 1 — Foundational (~0–2 Years): Governance and infrastructure readiness
Goal: Create an enabling institutional environment for the safe, equitable introduction of AI-enabled healthcare platforms.
Minimum conditions for Phase 1 completion include at least one interoperable regional data environment, a regulatory sandbox or controlled experimentation pathway, and validated workflow mapping for priority bottlenecks. These function as gate criteria for Phase 2 investment.
Key actions:
− Governance: Establish coordinated national AI in health governance linking demographic strategy with ethical and deployment oversight [1414Singapore Ministry of Health. Healthier SG: Envisioning our healthcare system's next bound. Singapore: MOH; 2022.,4141Ministerial Committee on Ageing. Action plan for successful ageing 2023 update. Singapore: MCA; 2023.].
− Data Infrastructure: Mandate HL7 FHIR adoption and secure federated architecture, positioning legacy migration as a capital investment rather than an operating expense [3030Rajpurkar P, Chen E, Banerjee O, Topol EJ. AI in health and medicine. Nat Med. 2022 Jan;28(1):31-38. doi: 10.1038/s41591-021-01614-0. Epub 2022 Jan 20. PMID: 35058619.].
− Regulation: Create regulatory sandboxes for supervised testing of adaptive AI systems and mandate post-deployment performance monitoring [3333European Commission. Regulation laying down harmonised rules on artificial intelligence (EU AI Act). Brussels: European Commission; 2024.].
− Public Engagement: Initiate early co-design with older adults’ caregivers and clinicians to build trust and inform workflow specifications [1919Cresswell K. NHS Scotland's decision support platform: a formative qualitative evaluation. BMJ Health Care Inform. 2020;27(1):e100033.].
Operational exit criteria for Phase 1 are detailed in Appendix D (Table D1).
Phase 2 — Pilot and validation (~2–5 Years): Targeted deployment and evidence generation
Goal: Generate rigorous, reproducible evidence on clinical effectiveness, workflow integration feasibility, and cost economics in high-need settings.
Key actions:
− Targeted Pilots: Prioritise deployment in structurally constrained settings, including rural elderly isolation and long-term care workforce shortages, while selecting sites with varying institutional readiness [66Kinsella K, Phillips DR. Global aging: the challenge of success. Popul Bull. 2005;60(1):1–40.].
− Evidence Standards: Employ rigorous study designs, including randomised trials where feasible, that follow CONSORT AI [4646CONSORT AI Steering Group. CONSORT AI extension for clinical trials. Nat Med. 2020;26:1364–1374.] and TRIPOD AI [4747TRIPOD AI Consortium. TRIPOD AI reporting guideline for prediction models [Internet]. 2023 [cited 2026 Apr 3]. Available from: https://www.tripod-statement.org/] guidance with prospective registration and adequate power for clinically meaningful outcomes.
− Workflow Redesign: Specify required workflow changes before deployment and recognise that neutral results without redesign indicate implementation misalignment rather than technological failure.
− User Adoption Monitoring: Treat adoption rates, workflow adherence, and clinician override frequency as primary implementation outcomes.
− Workforce Development: Integrate AI literacy and human AI collaboration training into professional education and budget training as a core pilot cost [1919Cresswell K. NHS Scotland's decision support platform: a formative qualitative evaluation. BMJ Health Care Inform. 2020;27(1):e100033.].
Structured validation metrics for Phase 2 are summarised in Appendix D (Table D2).
Phase 3 — Scaled deployment (~5–10 Years): Integration and system reform
Goal: Transition validated AI-enabled service platforms into routine, population-level healthcare delivery within reformed payment models and national data governance frameworks.
The transition from pilot to scale is historically the most failure-prone stage of digital health deployment [1717Greenhalgh T. Beyond adoption: the NASSS framework. J Med Internet Res. 2017;19(11).]. Scaled deployment should be conditional on Phase 2 evidence.
Key actions:
− National Rollout: Link procurement to demonstrate effectiveness and equity appraisal through health technology assessment bodies while sequencing expansion from sites with the highest digital readiness [3030Rajpurkar P, Chen E, Banerjee O, Topol EJ. AI in health and medicine. Nat Med. 2022 Jan;28(1):31-38. doi: 10.1038/s41591-021-01614-0. Epub 2022 Jan 20. PMID: 35058619.].
− Legacy Integration: Require interoperability with dominant national EHR systems as a procurement condition and fund system integration as core health infrastructure.
− Adaptive Surveillance: Mandate continuous monitoring for safety bias and performance drift in alignment with FDA and EU AI Act standards [3333European Commission. Regulation laying down harmonised rules on artificial intelligence (EU AI Act). Brussels: European Commission; 2024.,3636Obermeyer Z, Powers B, Vogeli C, Mullainathan S. Dissecting racial bias in an algorithm used to manage the health of populations. Science. 2019 Oct 25;366(6464):447-453. doi: 10.1126/science.aax2342. PMID: 31649194.].
− Payment Reform: Permanently aligned reimbursement with validated AI-enabled value-based care models, recognising that sustained scale depends on financing reform [88Organisation for Economic Co-operation and Development (OECD). Fiscal sustainability and population ageing: OECD economic outlook. Paris: OECD Publishing; 2023.].
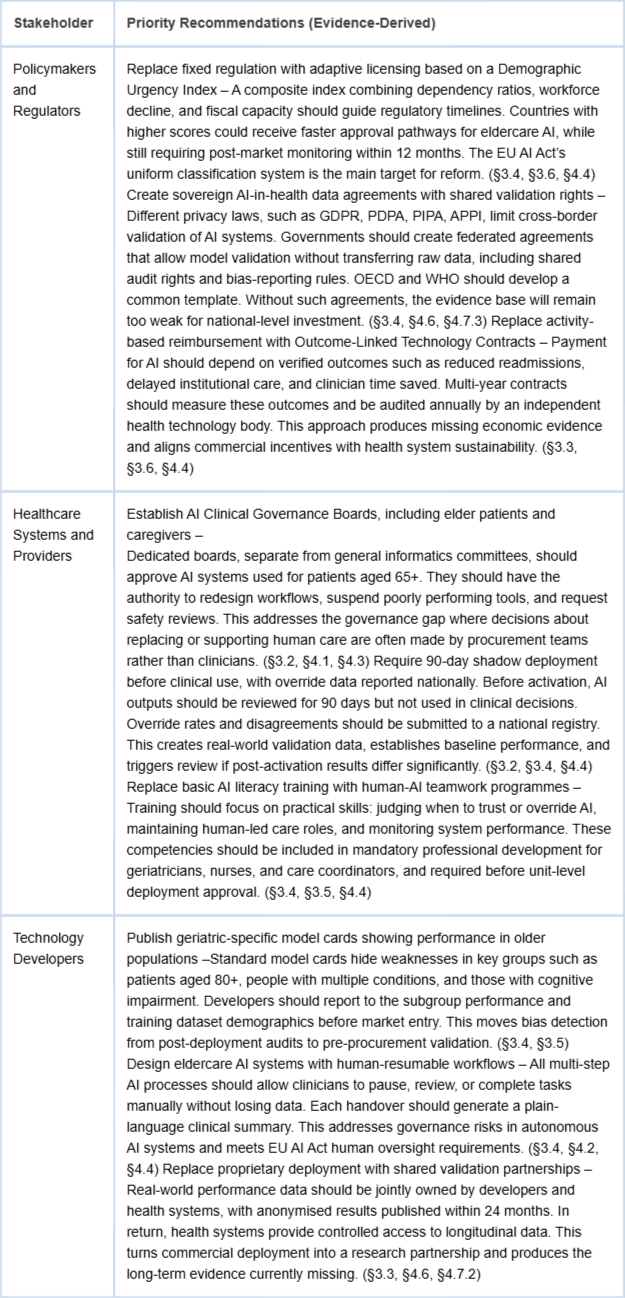
Stakeholder recommendations
AI implementation will fail if governance, provider institutions, and technology development advance independently. Recommendations below specify concrete mechanisms for each stakeholder group.
Table 8 synthesises the stakeholder-specific recommendations derived from the evidence base and discussion sections. It highlights how coordinated action across policy, provider, and technology domains is required to enable effective and scalable AI implementation in ageing health systems.
Table 8: Stakeholder Recommendations for AI Implementation in Ageing Health Systems.
Future research agenda
Sections 3.2 to 3.5 reveal three key research gaps. If these gaps remain, evidence will not grow fast enough to support ageing health systems. This agenda proposes three research tracks.
Track 1: Long-term clinical and economic evaluation
The largest gap is the lack of long-term evidence. Multiyear studies are needed to measure effects on healthy life expectancy, mortality, quality of life, and long-term healthcare costs in older populations. Economic impact is hard to measure for three reasons. Healthcare spending changes due to ageing wages and policy at the same time. Pilot projects often occur in high-capacity systems and may not reflect national conditions. Efficiency gains may also be offset by growing demand from ageing populations. Future studies should include economists from the start, use difference in differences methods that compare regions adopting AI at different times [88Organisation for Economic Co-operation and Development (OECD). Fiscal sustainability and population ageing: OECD economic outlook. Paris: OECD Publishing; 2023.,3838Organisation for Economic Co-operation and Development (OECD). Adapting health systems to an ageing population. Paris: OECD Publishing; 2024.], link health and social data, and compare results across countries using OECD data standards [77Ministry of Health, Labour and Welfare, Japan. Annual health, labour and welfare report 2023. Tokyo: MHLW; 2023.,3434Organisation for Economic Co-operation and Development (OECD). AI in health: Action plan for responsible deployment. Paris: OECD; 2024.]. Until stronger evidence exists, claims that AI will reduce healthcare spending should be treated cautiously.
Track 2: Institutional implementation research
AI implementation varies across countries due to governance, financing models, and digital infrastructure. However, research comparing these factors is limited. Studies should compare centralised and decentralised systems using common frameworks such as NASSS [1717Greenhalgh T. Beyond adoption: the NASSS framework. J Med Internet Res. 2017;19(11).] and CFIR [4848Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009 Aug 7;4:50. doi: 10.1186/1748-5908-4-50. PMID: 19664226; PMCID: PMC2736161.]. Research across early adopter countries, including Japan, South Korea, and Singapore, can provide lessons for later adopting countries such as Italy and France [3838Organisation for Economic Co-operation and Development (OECD). Adapting health systems to an ageing population. Paris: OECD Publishing; 2024.,3434Organisation for Economic Co-operation and Development (OECD). AI in health: Action plan for responsible deployment. Paris: OECD; 2024.]. Another key gap is how reimbursement and procurement systems affect adoption. Payment models often determine whether proven AI tools become funded healthcare services [88Organisation for Economic Co-operation and Development (OECD). Fiscal sustainability and population ageing: OECD economic outlook. Paris: OECD Publishing; 2023.,1414Singapore Ministry of Health. Healthier SG: Envisioning our healthcare system's next bound. Singapore: MOH; 2022.].
Track 3: Human–AI care integration
Efficiency gains may hide declines in human care quality. This risk is institutional rather than purely technical. Future studies should measure outcomes such as patient dignity, social connection, human contact time, and continuity of care in all Phase 2 pilots [2525Moyle W. Exploring the effect of companion robots on emotional expression in older adults with dementia. J Gerontol Nurs. 2017;43(5):27–35.,2626Moyle W, Jones CJ, Murfield JE, Thalib L, Beattie ERA, Shum DKH, O'Dwyer ST, Mervin MC, Draper BM. Use of a Robotic Seal as a Therapeutic Tool to Improve Dementia Symptoms: A Cluster-Randomized Controlled Trial. J Am Med Dir Assoc. 2017 Sep 1;18(9):766-773. doi: 10.1016/j.jamda.2017.03.018. Epub 2017 Aug 2. PMID: 28780395.]. Research should also examine how AI tools such as ambient documentation affect clinician attention, reasoning, and job satisfaction over time [2020Matheny ME, Whicher D, Thadaney Israni S. Artificial Intelligence in Health Care: A Report From the National Academy of Medicine. JAMA. 2020 Feb 11;323(6):509-510. doi: 10.1001/jama.2019.21579. PMID: 31845963.,3131Sinsky CA. Metrics for assessing physician activity using electronic health records: the Association of American Medical Colleges approach. J Am Med Inform Assoc. 2021;28(4):840–847.]. Caregiver impact is another important gap. Studies should assess whether ageing in place technologies reduce or shift informal caregiving burden within families [99Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, Brayne C, Burns A, Cohen-Mansfield J, Cooper C, Costafreda SG, Dias A, Fox N, Gitlin LN, Howard R, Kales HC, Kivimäki M, Larson EB, Ogunniyi A, Orgeta V, Ritchie K, Rockwood K, Sampson EL, Samus Q, Schneider LS, Selbæk G, Teri L, Mukadam N. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020 Aug 8;396(10248):413-446. doi: 10.1016/S0140-6736(20)30367-6. Epub 2020 Jul 30. Erratum in: Lancet. 2023 Sep 30;402(10408):1132. doi: 10.1016/S0140-6736(23)02043-3. PMID: 32738937; PMCID: PMC7392084.,3232Organisation for Economic Co-operation and Development (OECD). The economic benefit of promoting healthy ageing and community care. Paris: OECD Publishing; 2025.]. Together, these three research tracks form the evidence needed to turn the proposed roadmap into a tested policy framework.
Review methodology limitations: This study uses a structured narrative review with systematic elements to integrate evidence from multiple disciplines, including health policy, economics, artificial intelligence, and gerontology. Full PRISMA compliance was not achievable given the heterogeneous grey literature included. The review is better described as PRISMA-informed. A structured review protocol was developed before data extraction, but was not formally registered; readers should interpret findings accordingly, and future replication studies should register prospectively.
The evidence base is concentrated in high-resource, digitally mature health systems, which limits generalisability to lower capacity contexts. Most primary studies remain short-term pilot deployments, which restrict inference about sustained population-scale cost effectiveness. Consequently, the macroeconomic moderation hypothesis proposed in this paper remains unvalidated on the national scale.
Another limitation concerns the generalisability of AI systems. Many models are trained on specific clinical datasets and may not perform consistently across different populations, health systems, or care environments. Performance may vary due to differences in data quality, clinical practice patterns, demographic structure, and health system organisation. This heterogeneity limits the transferability of pilot results in broader healthcare contexts.
Implementation and infrastructure risks: Large-scale AI deployment requires substantial computational and energy infrastructure, often overlooked in health policy discussions. Capital costs for servers’ storage network upgrades and cooling infrastructure must therefore be included in health system investment planning. Jurisdictions such as the European Union and Singapore also operate under net-zero climate commitments, which may constrain the expansion of energy-intensive digital infrastructure without renewable energy sourcing.
Health systems may also face vendor locking risks when procuring AI platforms from a small number of dominant providers. Over time, this concentration may reduce strategic autonomy over clinical data infrastructure workflow design and procurement leverage, particularly under demographic pressure to scale solutions rapidly [4949Organisation for Economic Co-operation and Development (OECD). OECD digital government outlook 2023. Paris: OECD Publishing; 2023. doi:10.1787/1a89a067-en]. The OECD has noted that digital public infrastructure requires governance mechanisms that prevent monopolistic concentration in procurement markets [4949Organisation for Economic Co-operation and Development (OECD). OECD digital government outlook 2023. Paris: OECD Publishing; 2023. doi:10.1787/1a89a067-en]. Mitigation strategies include mandatory open API interoperability requirements, performance-linked contracts with independent audit rights, and phased pilot structures that preserve competitive tendering.
Global data governance constraints: Cross-border AI evaluation is constrained by fragmented international privacy and data governance frameworks. Regulations such as the European Union’s General Data Protection Regulation (GDPR) and the emerging European Health Data Space differ significantly from Singapore’s Personal Data Protection Act (PDPA), Japan’s Act on the Protection of Personal Information, and South Korea’s Personal Information Protection Act [3434Organisation for Economic Co-operation and Development (OECD). AI in health: Action plan for responsible deployment. Paris: OECD; 2024.,5050European Commission. Proposal for a regulation on the European Health Data Space. Brussels: European Commission; 2022.,5151Personal Information Protection Commission, Republic of Korea. Personal Information Protection Act (PIPA): consolidated text as amended 2023 [Internet]. Seoul: PIPC; 2023 [cited 2026 Apr 3]. Available from: https://www.pipc.go.kr/eng/]. These differences complicate cross-border model validation, federated learning, and multi-country evaluation designs identified as priorities in Section 4.6.
Until internationally coordinated frameworks for responsible cross-border health data exchange emerge, potentially under WHO or OECD leadership, the global evidence for AI-enabled healthcare will remain fragmented across jurisdictions. Taking together these limitations indicates that the roadmap proposed in this study should be interpreted as a governance-oriented implementation hypothesis that requires empirical validation through the research agenda outlined in Section 4.6.
Policy impact and potential policy outcomes: Section 4.5 outlines the institutional responsibilities of policymakers, healthcare systems, and technology developers. This section considers the system-level outcomes that could plausibly follow from implementation of the proposed roadmap. While validated macroeconomic proof is not yet available, the evidence reviewed provides a reasonable basis for estimating potential policy impact.
Healthcare system outcomes
Avoidable admissions: Remote monitoring has demonstrated 20% - 30% reductions in emergency utilisation in structured pilots [2222Steventon A, Bardsley M, Billings J, Dixon J, Doll H, Hirani S, Cartwright M, Rixon L, Knapp M, Henderson C, Rogers A, Fitzpatrick R, Hendy J, Newman S; Whole System Demonstrator Evaluation Team. Effect of telehealth on use of secondary care and mortality: findings from the Whole System Demonstrator cluster randomised trial. BMJ. 2012 Jun 21;344:e3874. doi: 10.1136/bmj.e3874. PMID: 22723612; PMCID: PMC3381047.,2323Klersy C, De Silvestri A, Gabutti G, Regoli F, Auricchio A. A meta-analysis of remote monitoring of heart failure patients. J Am Coll Cardiol. 2009 Oct 27;54(18):1683-94. doi: 10.1016/j.jacc.2009.08.017. Erratum in: J Am Coll Cardiol. 2010 May 11;55(19):2185. PMID: 19850208.]. Evidence is moderate at the pilot level and plausible at the population level.
Clinician administrative burden: Ambient documentation has shown potential to reduce documentation time by at least 15 percent and may increase patient-facing time [3131Sinsky CA. Metrics for assessing physician activity using electronic health records: the Association of American Medical Colleges approach. J Am Med Inform Assoc. 2021;28(4):840–847.]. Evidence is emerging and mainly observational.
Early deterioration detection: Validated AI algorithms may enable earlier escalation of care, which could reduce the severity and cost of acute episodes [2222Steventon A, Bardsley M, Billings J, Dixon J, Doll H, Hirani S, Cartwright M, Rixon L, Knapp M, Henderson C, Rogers A, Fitzpatrick R, Hendy J, Newman S; Whole System Demonstrator Evaluation Team. Effect of telehealth on use of secondary care and mortality: findings from the Whole System Demonstrator cluster randomised trial. BMJ. 2012 Jun 21;344:e3874. doi: 10.1136/bmj.e3874. PMID: 22723612; PMCID: PMC3381047.,2323Klersy C, De Silvestri A, Gabutti G, Regoli F, Auricchio A. A meta-analysis of remote monitoring of heart failure patients. J Am Coll Cardiol. 2009 Oct 27;54(18):1683-94. doi: 10.1016/j.jacc.2009.08.017. Erratum in: J Am Coll Cardiol. 2010 May 11;55(19):2185. PMID: 19850208.]. Evidence moderates structured settings and emerges in community eldercare.
Care coordination: The Autonomous Orchestration pillar of AAF 3.0 could potentially reduce fragmented specialist management in interoperable systems. Evidence emerging through the mechanism is theoretically grounded within Phase 3 horizons [1717Greenhalgh T. Beyond adoption: the NASSS framework. J Med Internet Res. 2017;19(11).,2020Matheny ME, Whicher D, Thadaney Israni S. Artificial Intelligence in Health Care: A Report From the National Academy of Medicine. JAMA. 2020 Feb 11;323(6):509-510. doi: 10.1001/jama.2019.21579. PMID: 31845963.].
Economic outcomes
Healthcare expenditure moderation: If AI interventions reduced projected expenditure growth by 5 to 10 percent relative to IMF projections [1010International Monetary Fund (IMF). Fiscal monitor, April 2024. Washington (DC): IMF; 2024.], advanced economies could potentially avoid about 0.1 to 0.35 percentage points of GDP annually by mid-century. The scenario is based on plausible extrapolation from moderate micro-level evidence and is not a validated projection.
Workforce productivity: AI-supported documentation and coordination may increase the effective capacity of care workers by roughly 10 to 20 percent under optimistic but plausible conditions, which could partially offset Japan's projected workforce shortfall [66Kinsella K, Phillips DR. Global aging: the challenge of success. Popul Bull. 2005;60(1):1–40.,3131Sinsky CA. Metrics for assessing physician activity using electronic health records: the Association of American Medical Colleges approach. J Am Med Inform Assoc. 2021;28(4):840–847.].
Long-term care costs: Delaying institutionalisation by six to twelve months through ageing in place technologies could generate substantial individual long-term care savings [3232Organisation for Economic Co-operation and Development (OECD). The economic benefit of promoting healthy ageing and community care. Paris: OECD Publishing; 2025.]. Evidence is moderate at the individual level but dependent on population-scale adoption.
Workforce and social outcomes
Workforce shortage mitigation: AI workflow tools may extend staff productivity and reduce burnout-related attrition in geriatric care settings [3131Sinsky CA. Metrics for assessing physician activity using electronic health records: the Association of American Medical Colleges approach. J Am Med Inform Assoc. 2021;28(4):840–847.,5252World Health Organization. Health and care workforce: the time to act is now. Geneva: WHO; 2023.]. Evidence is plausible with partial empirical support.
Ageing in place: Integrated remote monitoring and community care may extend independent living, reduce institutional demand, and improve wellbeing [3232Organisation for Economic Co-operation and Development (OECD). The economic benefit of promoting healthy ageing and community care. Paris: OECD Publishing; 2025.,3838Organisation for Economic Co-operation and Development (OECD). Adapting health systems to an ageing population. Paris: OECD Publishing; 2024.]. Evidence is moderate but dependent on system design.
Caregiver burden and rural access: AI-enabled telehealth may expand geographic access to care and could reduce caregiving pressure on family networks. Evidence remains emerging and requires further evaluation.
These potential outcomes support investment in the phased roadmap even under conservative assumptions. Healthcare and social benefits are supported by evidence from controlled settings, while economic impacts require the longitudinal research programme described in Section 4.6 to move from plausible scenarios to validated projections [5555Organisation for Economic Co-operation and Development (OECD). Society at a glance 2024. Paris: OECD Publishing; 2024.-5757Maestas N, Mullen KJ, Powell D. The effect of population aging on economic growth, the labor force, and productivity. Am Econ J Macroecon. 2023;15(2):306–332. doi:10.1257/mac.20190196]..
This structured narrative review with systematic elements examined 81 sources published between 2020 and 2025, synthesising evidence across demography, health economics, implementation science, and AI research to evaluate the potential role of AI, including emerging agentic AI architectures, in addressing the structural pressures of demographic ageing in advanced economies. Drawing on the NASSS sociotechnical framework and a cross-disciplinary synthesis, the review assessed five principal AI application domains: remote monitoring, assistive robotics, diagnostic support, medication adherence, and workflow automation, alongside the governance, regulatory, financial, and infrastructural conditions that determine whether technical capability translates into population-level benefit. The AAF 3.0 domain-mapping matrix is presented as a conceptual implementation tool linking AI capabilities to specific system pressures across present, near-term, and speculative horizons, and a phased sociotechnical roadmap is proposed to integrate governance sequencing, reimbursement reform, and equity safeguards within a ten-year implementation horizon.
A consistent finding across the reviewed literature is that system-level impact is constrained more reliably by institutional factors than by technical performance. The inverse evidence–complexity relationship identified in this review demonstrates that the AI applications most needed in ageing health systems, particularly care coordination and social isolation interventions, carry the weakest evidence base, while foundational applications such as diagnostic imaging AI benefit from stronger but narrower evidence. Macroeconomic fiscal moderation remains empirically unvalidated at the national scale, and AI should therefore be understood neither as a substitute for demographic policy nor as a self-executing technological solution. Its potential contribution depends on alignment between governance, reimbursement models, interoperability standards, and workforce structures, so that augmentation technologies can be integrated without degrading relational care or widening existing health inequities. Singapore’s coordinated, governance-first strategy illustrates that pre-emptive institutional alignment, across prevention, financing, workforce, and digital infrastructure, can serve as a useful benchmark for sequencing reform before demographic pressures peak.
The phased sociotechnical roadmap presented here positions AI adoption within a governance-sequencing framework, recognising institutional reform rather than algorithmic capability as the primary constraint for sustainable scale. The three-track research agenda outlined in Section 4.6, spanning long-term clinical and economic evaluation, comparative implementation research, and human–AI care integration, identifies the longitudinal and comparative evidence required to move AI deployment in eldercare from a plausible conceptual hypothesis to a more empirically validated policy instrument. Structural constraints, including energy infrastructure requirements, vendor dependency risks, and fragmented international data governance frameworks, should be incorporated into implementation planning from the outset. Ultimately, the future of ageing societies will depend less on what AI systems can potentially do than on whether institutions are prepared to deploy them responsibly, equitably, and sustainably.
The authors, Dr. Rachel Ooi and Baskar Periasamy, gratefully acknowledge the encouragement and support of their families, colleagues, and the wider research community during the preparation of this review. The authors also thank the many researchers whose work and contributions in this field have helped advance similar directions of inquiry.
United Nations, Department of Economic and Social Affairs, Population Division. World population prospects 2024. New York: United Nations; 2024.
Organisation for Economic Co-operation and Development (OECD). Health at a glance 2023: OECD indicators. Paris: OECD Publishing; 2023. doi:10.1787/7a7afb35-en
Statistics Korea. 2023 birth statistics. Daejeon: Statistics Korea; 2024.
World Health Organization. World health statistics 2024. Geneva: WHO; 2024.
United Nations. World population ageing 2019: Highlights. New York: United Nations; 2019.
Kinsella K, Phillips DR. Global aging: the challenge of success. Popul Bull. 2005;60(1):1–40.
Ministry of Health, Labour and Welfare, Japan. Annual health, labour and welfare report 2023. Tokyo: MHLW; 2023.
Organisation for Economic Co-operation and Development (OECD). Fiscal sustainability and population ageing: OECD economic outlook. Paris: OECD Publishing; 2023.
Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, Brayne C, Burns A, Cohen-Mansfield J, Cooper C, Costafreda SG, Dias A, Fox N, Gitlin LN, Howard R, Kales HC, Kivimäki M, Larson EB, Ogunniyi A, Orgeta V, Ritchie K, Rockwood K, Sampson EL, Samus Q, Schneider LS, Selbæk G, Teri L, Mukadam N. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020 Aug 8;396(10248):413-446. doi: 10.1016/S0140-6736(20)30367-6. Epub 2020 Jul 30. Erratum in: Lancet. 2023 Sep 30;402(10408):1132. doi: 10.1016/S0140-6736(23)02043-3. PMID: 32738937; PMCID: PMC7392084.
International Monetary Fund (IMF). Fiscal monitor, April 2024. Washington (DC): IMF; 2024.
Singapore Ministry of Health. Committee of Supply Debate 2024 — Healthcare statistics. Singapore: MOH; 2024.
International Monetary Fund (IMF). Working paper WP/23/75: The economic impact of ageing populations. Washington (DC): IMF; 2023.
Vlandas T. The political economy of pension reform in France. J Eur Soc Policy. 2024;34(1):12–28.
Singapore Ministry of Health. Healthier SG: Envisioning our healthcare system's next bound. Singapore: MOH; 2022.
AARP Public Policy Institute. Global aging readiness index 2024. Washington (DC): AARP; 2024.
Wang L. A survey on large language model-based autonomous agents. Front Comput Sci. 2024;18(6):1–26.
Greenhalgh T. Beyond adoption: the NASSS framework. J Med Internet Res. 2017;19(11).
European Commission. The 2024 ageing report: Economic and budgetary projections for EU member states. Luxembourg: Publications Office of the European Union; 2024.
Cresswell K. NHS Scotland's decision support platform: a formative qualitative evaluation. BMJ Health Care Inform. 2020;27(1):e100033.
Matheny ME, Whicher D, Thadaney Israni S. Artificial Intelligence in Health Care: A Report From the National Academy of Medicine. JAMA. 2020 Feb 11;323(6):509-510. doi: 10.1001/jama.2019.21579. PMID: 31845963.
Kelly CJ. Key challenges for delivering clinical impact with artificial intelligence. Nat Med. 2019;25(1):44–56.
Steventon A, Bardsley M, Billings J, Dixon J, Doll H, Hirani S, Cartwright M, Rixon L, Knapp M, Henderson C, Rogers A, Fitzpatrick R, Hendy J, Newman S; Whole System Demonstrator Evaluation Team. Effect of telehealth on use of secondary care and mortality: findings from the Whole System Demonstrator cluster randomised trial. BMJ. 2012 Jun 21;344:e3874. doi: 10.1136/bmj.e3874. PMID: 22723612; PMCID: PMC3381047.
Klersy C, De Silvestri A, Gabutti G, Regoli F, Auricchio A. A meta-analysis of remote monitoring of heart failure patients. J Am Coll Cardiol. 2009 Oct 27;54(18):1683-94. doi: 10.1016/j.jacc.2009.08.017. Erratum in: J Am Coll Cardiol. 2010 May 11;55(19):2185. PMID: 19850208.
Wada K. Robot therapy for dementia patients. Proc World Acad Sci Eng Technol. 2008;31:543–548.
Moyle W. Exploring the effect of companion robots on emotional expression in older adults with dementia. J Gerontol Nurs. 2017;43(5):27–35.
Moyle W, Jones CJ, Murfield JE, Thalib L, Beattie ERA, Shum DKH, O'Dwyer ST, Mervin MC, Draper BM. Use of a Robotic Seal as a Therapeutic Tool to Improve Dementia Symptoms: A Cluster-Randomized Controlled Trial. J Am Med Dir Assoc. 2017 Sep 1;18(9):766-773. doi: 10.1016/j.jamda.2017.03.018. Epub 2017 Aug 2. PMID: 28780395.
Esteva A, Kuprel B, Novoa RA, Ko J, Swetter SM, Blau HM, Thrun S. Dermatologist-level classification of skin cancer with deep neural networks. Nature. 2017 Feb 2;542(7639):115-118. doi: 10.1038/nature21056. Epub 2017 Jan 25. Erratum in: Nature. 2017 Jun 28;546(7660):686. doi: 10.1038/nature22985. PMID: 28117445; PMCID: PMC8382232.
Rajpurkar P. CheXNet: Radiologist-level pneumonia detection on chest X-rays with deep learning. arXiv. 2017;arXiv:1711.05225.
Liu X. A comparison of deep learning performance against healthcare professionals. Nat Med. 2019;25(6):1009–1015.
Rajpurkar P, Chen E, Banerjee O, Topol EJ. AI in health and medicine. Nat Med. 2022 Jan;28(1):31-38. doi: 10.1038/s41591-021-01614-0. Epub 2022 Jan 20. PMID: 35058619.
Sinsky CA. Metrics for assessing physician activity using electronic health records: the Association of American Medical Colleges approach. J Am Med Inform Assoc. 2021;28(4):840–847.
Organisation for Economic Co-operation and Development (OECD). The economic benefit of promoting healthy ageing and community care. Paris: OECD Publishing; 2025.
European Commission. Regulation laying down harmonised rules on artificial intelligence (EU AI Act). Brussels: European Commission; 2024.
Organisation for Economic Co-operation and Development (OECD). AI in health: Action plan for responsible deployment. Paris: OECD; 2024.
Meskó B, Topol EJ. The imperative for regulatory oversight of large language models (or generative AI) in healthcare. NPJ Digit Med. 2023 Jul 6;6(1):120. doi: 10.1038/s41746-023-00873-0. PMID: 37414860; PMCID: PMC10326069.
Obermeyer Z, Powers B, Vogeli C, Mullainathan S. Dissecting racial bias in an algorithm used to manage the health of populations. Science. 2019 Oct 25;366(6464):447-453. doi: 10.1126/science.aax2342. PMID: 31649194.
Organisation for Economic Co-operation and Development (OECD), European Commission. Health at a glance: Europe 2024. Paris: OECD Publishing; 2024.
Organisation for Economic Co-operation and Development (OECD). Adapting health systems to an ageing population. Paris: OECD Publishing; 2024.
Statistics Korea. Population projections for Korea. Seoul: Statistics Korea; 2023.
Singapore Ministry of Health. Action plan for successful ageing. Singapore: MOH; 2023.
Ministerial Committee on Ageing. Action plan for successful ageing 2023 update. Singapore: MCA; 2023.
Ministry of Health Singapore (MOH). Healthier SG white paper 2022. Singapore: MOH; 2022.
Ministry of Health Singapore (MOH). Healthcare financing white paper 2023. Singapore: MOH; 2023.
Ministry of Manpower Singapore (MOM). Labour force in Singapore 2023. Singapore: MOM; 2023.
Integrated Health Information Systems (IHiS). Digital health blueprint 2023. Singapore: IHiS; 2023.
CONSORT AI Steering Group. CONSORT AI extension for clinical trials. Nat Med. 2020;26:1364–1374.
TRIPOD AI Consortium. TRIPOD AI reporting guideline for prediction models [Internet]. 2023 [cited 2026 Apr 3]. Available from: https://www.tripod-statement.org/
Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009 Aug 7;4:50. doi: 10.1186/1748-5908-4-50. PMID: 19664226; PMCID: PMC2736161.
Organisation for Economic Co-operation and Development (OECD). OECD digital government outlook 2023. Paris: OECD Publishing; 2023. doi:10.1787/1a89a067-en
European Commission. Proposal for a regulation on the European Health Data Space. Brussels: European Commission; 2022.
Personal Information Protection Commission, Republic of Korea. Personal Information Protection Act (PIPA): consolidated text as amended 2023 [Internet]. Seoul: PIPC; 2023 [cited 2026 Apr 3]. Available from: https://www.pipc.go.kr/eng/
World Health Organization. Health and care workforce: the time to act is now. Geneva: WHO; 2023.
Björnsson B, Borrebaeck C, Elander N, Gasslander T, Gawel DR, Gustafsson M, Jörnsten R, Lee EJ, Li X, Lilja S, Martínez-Enguita D, Matussek A, Sandström P, Schäfer S, Stenmarker M, Sun XF, Sysoev O, Zhang H, Benson M; Swedish Digital Twin Consortium. Digital twins to personalize medicine. Genome Med. 2019 Dec 31;12(1):4. doi: 10.1186/s13073-019-0701-3. PMID: 31892363; PMCID: PMC6938608.
Raghu A. Deep reinforcement learning for sepsis treatment. arXiv. 2017;arXiv:1711.09602.
Organisation for Economic Co-operation and Development (OECD). Society at a glance 2024. Paris: OECD Publishing; 2024.
Ministry of Health, Singapore. Speech by Mr Ong Ye Kung, Minister for Health, at the MOH Committee of Supply Debate 2025. Singapore: MOH; 2025.
Maestas N, Mullen KJ, Powell D. The effect of population aging on economic growth, the labor force, and productivity. Am Econ J Macroecon. 2023;15(2):306–332. doi:10.1257/mac.20190196
Ooi R, Periasamy B. Agentic AI for Ageing Healthcare Systems in Advanced Economies: A Structured Review of Evidence, Institutional Barriers, and a Sociotechnical Implementation Roadmap. IgMin Res. March 31, 2026; 4(3): 094-109. IgMin ID: igmin337; DOI:10.61927/igmin337; Available at: igmin.link/p337
1Founder of Antioch Streams; Global AI Ambassador & Singapore Chapter Co-Founder (GCRAI); Adjunct Associate Professor (NTU Singapore); ExD Master Coach, Singapore Management University, Singapore
2CISSP (Certified Information Systems Security Professional); Associate Researcher, Antioch Streams, Singapore Management University, Singapore
Address Correspondence: Dr. Rachel Ooi, Founder of Antioch Streams; Global AI Ambassador & Singapore Chapter Co-Founder (GCRAI); Adjunct Associate Professor (NTU Singapore); ExD Master Coach, Singapore Management University, Singapore, Email: [email protected]
How to cite this article: Ooi R, Periasamy B. Agentic AI for Ageing Healthcare Systems in Advanced Economies: A Structured Review of Evidence, Institutional Barriers, and a Sociotechnical Implementation Roadmap. IgMin Res. March 31, 2026; 4(3): 094-109. IgMin ID: igmin337; DOI:10.61927/igmin337; Available at: igmin.link/p337
Copyright: 2026 Ooi R, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Table 8: Stakeholder Recommendations for AI Implementation ...
United Nations, Department of Economic and Social Affairs, Population Division. World population prospects 2024. New York: United Nations; 2024.
Organisation for Economic Co-operation and Development (OECD). Health at a glance 2023: OECD indicators. Paris: OECD Publishing; 2023. doi:10.1787/7a7afb35-en
Statistics Korea. 2023 birth statistics. Daejeon: Statistics Korea; 2024.
World Health Organization. World health statistics 2024. Geneva: WHO; 2024.
United Nations. World population ageing 2019: Highlights. New York: United Nations; 2019.
Kinsella K, Phillips DR. Global aging: the challenge of success. Popul Bull. 2005;60(1):1–40.
Ministry of Health, Labour and Welfare, Japan. Annual health, labour and welfare report 2023. Tokyo: MHLW; 2023.
Organisation for Economic Co-operation and Development (OECD). Fiscal sustainability and population ageing: OECD economic outlook. Paris: OECD Publishing; 2023.
Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, Brayne C, Burns A, Cohen-Mansfield J, Cooper C, Costafreda SG, Dias A, Fox N, Gitlin LN, Howard R, Kales HC, Kivimäki M, Larson EB, Ogunniyi A, Orgeta V, Ritchie K, Rockwood K, Sampson EL, Samus Q, Schneider LS, Selbæk G, Teri L, Mukadam N. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020 Aug 8;396(10248):413-446. doi: 10.1016/S0140-6736(20)30367-6. Epub 2020 Jul 30. Erratum in: Lancet. 2023 Sep 30;402(10408):1132. doi: 10.1016/S0140-6736(23)02043-3. PMID: 32738937; PMCID: PMC7392084.
International Monetary Fund (IMF). Fiscal monitor, April 2024. Washington (DC): IMF; 2024.
Singapore Ministry of Health. Committee of Supply Debate 2024 — Healthcare statistics. Singapore: MOH; 2024.
International Monetary Fund (IMF). Working paper WP/23/75: The economic impact of ageing populations. Washington (DC): IMF; 2023.
Vlandas T. The political economy of pension reform in France. J Eur Soc Policy. 2024;34(1):12–28.
Singapore Ministry of Health. Healthier SG: Envisioning our healthcare system's next bound. Singapore: MOH; 2022.
AARP Public Policy Institute. Global aging readiness index 2024. Washington (DC): AARP; 2024.
Wang L. A survey on large language model-based autonomous agents. Front Comput Sci. 2024;18(6):1–26.
Greenhalgh T. Beyond adoption: the NASSS framework. J Med Internet Res. 2017;19(11).
European Commission. The 2024 ageing report: Economic and budgetary projections for EU member states. Luxembourg: Publications Office of the European Union; 2024.
Cresswell K. NHS Scotland's decision support platform: a formative qualitative evaluation. BMJ Health Care Inform. 2020;27(1):e100033.
Matheny ME, Whicher D, Thadaney Israni S. Artificial Intelligence in Health Care: A Report From the National Academy of Medicine. JAMA. 2020 Feb 11;323(6):509-510. doi: 10.1001/jama.2019.21579. PMID: 31845963.
Kelly CJ. Key challenges for delivering clinical impact with artificial intelligence. Nat Med. 2019;25(1):44–56.
Steventon A, Bardsley M, Billings J, Dixon J, Doll H, Hirani S, Cartwright M, Rixon L, Knapp M, Henderson C, Rogers A, Fitzpatrick R, Hendy J, Newman S; Whole System Demonstrator Evaluation Team. Effect of telehealth on use of secondary care and mortality: findings from the Whole System Demonstrator cluster randomised trial. BMJ. 2012 Jun 21;344:e3874. doi: 10.1136/bmj.e3874. PMID: 22723612; PMCID: PMC3381047.
Klersy C, De Silvestri A, Gabutti G, Regoli F, Auricchio A. A meta-analysis of remote monitoring of heart failure patients. J Am Coll Cardiol. 2009 Oct 27;54(18):1683-94. doi: 10.1016/j.jacc.2009.08.017. Erratum in: J Am Coll Cardiol. 2010 May 11;55(19):2185. PMID: 19850208.
Wada K. Robot therapy for dementia patients. Proc World Acad Sci Eng Technol. 2008;31:543–548.
Moyle W. Exploring the effect of companion robots on emotional expression in older adults with dementia. J Gerontol Nurs. 2017;43(5):27–35.
Moyle W, Jones CJ, Murfield JE, Thalib L, Beattie ERA, Shum DKH, O'Dwyer ST, Mervin MC, Draper BM. Use of a Robotic Seal as a Therapeutic Tool to Improve Dementia Symptoms: A Cluster-Randomized Controlled Trial. J Am Med Dir Assoc. 2017 Sep 1;18(9):766-773. doi: 10.1016/j.jamda.2017.03.018. Epub 2017 Aug 2. PMID: 28780395.
Esteva A, Kuprel B, Novoa RA, Ko J, Swetter SM, Blau HM, Thrun S. Dermatologist-level classification of skin cancer with deep neural networks. Nature. 2017 Feb 2;542(7639):115-118. doi: 10.1038/nature21056. Epub 2017 Jan 25. Erratum in: Nature. 2017 Jun 28;546(7660):686. doi: 10.1038/nature22985. PMID: 28117445; PMCID: PMC8382232.
Rajpurkar P. CheXNet: Radiologist-level pneumonia detection on chest X-rays with deep learning. arXiv. 2017;arXiv:1711.05225.
Liu X. A comparison of deep learning performance against healthcare professionals. Nat Med. 2019;25(6):1009–1015.
Rajpurkar P, Chen E, Banerjee O, Topol EJ. AI in health and medicine. Nat Med. 2022 Jan;28(1):31-38. doi: 10.1038/s41591-021-01614-0. Epub 2022 Jan 20. PMID: 35058619.
Sinsky CA. Metrics for assessing physician activity using electronic health records: the Association of American Medical Colleges approach. J Am Med Inform Assoc. 2021;28(4):840–847.
Organisation for Economic Co-operation and Development (OECD). The economic benefit of promoting healthy ageing and community care. Paris: OECD Publishing; 2025.
European Commission. Regulation laying down harmonised rules on artificial intelligence (EU AI Act). Brussels: European Commission; 2024.
Organisation for Economic Co-operation and Development (OECD). AI in health: Action plan for responsible deployment. Paris: OECD; 2024.
Meskó B, Topol EJ. The imperative for regulatory oversight of large language models (or generative AI) in healthcare. NPJ Digit Med. 2023 Jul 6;6(1):120. doi: 10.1038/s41746-023-00873-0. PMID: 37414860; PMCID: PMC10326069.
Obermeyer Z, Powers B, Vogeli C, Mullainathan S. Dissecting racial bias in an algorithm used to manage the health of populations. Science. 2019 Oct 25;366(6464):447-453. doi: 10.1126/science.aax2342. PMID: 31649194.
Organisation for Economic Co-operation and Development (OECD), European Commission. Health at a glance: Europe 2024. Paris: OECD Publishing; 2024.
Organisation for Economic Co-operation and Development (OECD). Adapting health systems to an ageing population. Paris: OECD Publishing; 2024.
Statistics Korea. Population projections for Korea. Seoul: Statistics Korea; 2023.
Singapore Ministry of Health. Action plan for successful ageing. Singapore: MOH; 2023.
Ministerial Committee on Ageing. Action plan for successful ageing 2023 update. Singapore: MCA; 2023.
Ministry of Health Singapore (MOH). Healthier SG white paper 2022. Singapore: MOH; 2022.
Ministry of Health Singapore (MOH). Healthcare financing white paper 2023. Singapore: MOH; 2023.
Ministry of Manpower Singapore (MOM). Labour force in Singapore 2023. Singapore: MOM; 2023.
Integrated Health Information Systems (IHiS). Digital health blueprint 2023. Singapore: IHiS; 2023.
CONSORT AI Steering Group. CONSORT AI extension for clinical trials. Nat Med. 2020;26:1364–1374.
TRIPOD AI Consortium. TRIPOD AI reporting guideline for prediction models [Internet]. 2023 [cited 2026 Apr 3]. Available from: https://www.tripod-statement.org/
Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009 Aug 7;4:50. doi: 10.1186/1748-5908-4-50. PMID: 19664226; PMCID: PMC2736161.
Organisation for Economic Co-operation and Development (OECD). OECD digital government outlook 2023. Paris: OECD Publishing; 2023. doi:10.1787/1a89a067-en
European Commission. Proposal for a regulation on the European Health Data Space. Brussels: European Commission; 2022.
Personal Information Protection Commission, Republic of Korea. Personal Information Protection Act (PIPA): consolidated text as amended 2023 [Internet]. Seoul: PIPC; 2023 [cited 2026 Apr 3]. Available from: https://www.pipc.go.kr/eng/
World Health Organization. Health and care workforce: the time to act is now. Geneva: WHO; 2023.
Björnsson B, Borrebaeck C, Elander N, Gasslander T, Gawel DR, Gustafsson M, Jörnsten R, Lee EJ, Li X, Lilja S, Martínez-Enguita D, Matussek A, Sandström P, Schäfer S, Stenmarker M, Sun XF, Sysoev O, Zhang H, Benson M; Swedish Digital Twin Consortium. Digital twins to personalize medicine. Genome Med. 2019 Dec 31;12(1):4. doi: 10.1186/s13073-019-0701-3. PMID: 31892363; PMCID: PMC6938608.
Raghu A. Deep reinforcement learning for sepsis treatment. arXiv. 2017;arXiv:1711.09602.
Organisation for Economic Co-operation and Development (OECD). Society at a glance 2024. Paris: OECD Publishing; 2024.
Ministry of Health, Singapore. Speech by Mr Ong Ye Kung, Minister for Health, at the MOH Committee of Supply Debate 2025. Singapore: MOH; 2025.
Maestas N, Mullen KJ, Powell D. The effect of population aging on economic growth, the labor force, and productivity. Am Econ J Macroecon. 2023;15(2):306–332. doi:10.1257/mac.20190196
Agentic AI for Ageing Healthcare Systems in Advanced Economies: A Structured Review of Evidence, Institutional Barriers, and a Sociotechnical Implementation Roadmap


 Scan and get link
Scan and get link