IGMIN: We're glad you're here. Please click 'create a new query' if you are a new visitor to our website and need further information from us.
If you are already a member of our network and need to keep track of any developments regarding a question you have already submitted, click 'take me to my Query.'
Welcome to IgMin Research – an Open Access journal uniting Biology, Medicine, and Engineering. We’re dedicated to advancing global knowledge and fostering collaboration across scientific fields.
At IgMin Research, we bridge the frontiers of Biology, Medicine, and Engineering to foster interdisciplinary innovation. Our expanded scope now embraces a wide spectrum of scientific disciplines, empowering global researchers to explore, contribute, and collaborate through open access.
Welcome to IgMin, a leading platform dedicated to enhancing knowledge dissemination and professional growth across multiple fields of science, technology, and the humanities. We believe in the power of open access, collaboration, and innovation. Our goal is to provide individuals and organizations with the tools they need to succeed in the global knowledge economy.
IgMin Publications Inc., Suite 102, West Hartford, CT - 06110, USA
Background: Recently, the amount of bleeding during and after Total Hip Arthroplasty (THA) has decreased owing to the use of tranexamic acid, advancements in surgical devices, improvements in surgical skills, and the introduction of minimally invasive surgery. Therefore, the need for blood transfusions is decreasing. We monitored haemoglobin (Hb) and haematocrit (Ht) levels, estimated blood loss, transfusion rates, and other aspects of Anterolateral Supine THA (ALS-THA) performed at our institution without autologous blood donation and closed suction drainage.
Methods: Patients (n = 316) with preoperative Hb ≥10.0 g/dL during primary unilateral THA performed at our hospital from May 2021 to July 2023 were included. Hb and Ht levels, surgical time, intraoperative blood loss, estimated postoperative blood loss, allogeneic blood transfusion rates, and complication rates were evaluated. We performed logistic regression analysis on age, sex, blood type, height, weight, BMI, preoperative Hb, and preoperative Ht to evaluate the risk of blood transfusion. Receiver Operating Characteristic (ROC) analysis was performed on preoperative Hb levels and blood transfusions.
Results: Blood transfusions were performed in 10 of the 316 cases (3.2%), with a transfusion rate of 16.7% in patients with preoperative Hb < 12g/dL. Univariate analysis revealed significant differences in preoperative Hb and Ht levels, whereas multivariate analysis showed a significant difference in preoperative Hb (odds ratio 0.39). In ROC analysis, the cutoff value was Hb 12.3 g/dL (sensitivity 0.7; specificity 0.84).
Conclusion: The preoperative Hb level was the most important factor contributing to the transfusion risk in THA. Preoperative anemia treatment may further reduce blood transfusions.
During the 1980s and 1990s, the standard method of blood management in joint replacement shifted from allogeneic blood transfusions to autologous blood donations. However, in the late 1990s, reports began to surface questioning the necessity of autologous blood donation due to factors such as cost, inconvenience, hygiene, anaemia caused by blood loss, and ambiguous eligibility criteria [11Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB. Ananalysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am. 1999;81:2-10. PMID: 9973048-33Pierson JL, Hannon TJ, Earles DR. A blood conservation algorithm to reduce blood transfusions after total hip and knee arthroplasty. J Bone Joint Surg Am. 2004;87:1512-1518. PMID: 15252101]. Furthermore, advancements in surgical techniques, the use of tranexamic acid, the introduction of minimally invasive surgery, and improvements in surgical devices, have led to a decrease in both intra- and postoperative bleeding [44Sinclair ST, Warren JA, Murray TG, Bloomfield MR, McLaughlin JP, Piuzzi NS. Blood management in total hip arthroplasty: a nationwide trend analysis from 2011 to 2018. Eur J Orthop Surg Traumatol. 2023;33:45-50. PMID: 34714392]. Therefore, the need for autologous blood donations is decreasing [55Alvarez JC, Santiveri FX, Ramos I, Vela E, Puig L, Escolano F. Tranexamic acid reduces blood transfusion in total knee arthroplasty even when a blood conservation program is applied. Transfusion. 2008;48:519-525. PMID: 18067499-99Widman J, Jacobsson H, Larsson SA, Isacson J. No effect of drains on thepostoperative hematoma volume in hip replacement surgery. A randomized study using scintigraphy. Acta Orthop Scand. 2002;73:625-629. PMID: 12553508]. While closed drains have typically been used to reduce dead space and prevent haematomas, recent studies have reported risks of infection and delays in rehabilitation associated with their use, thereby challenging whether closed suction drainage is needed in THA [1010Parker MJ, Roberts CP, Hay D. Closed suction drainage for hip and knee arthroplasty. A meta-analysis. J Bone Joint Surg Am.2004;86:1146-1152. PMID: 15173286-1212Migliorini F, Maffulli N, Betsch M, Eschweiler J, Tingart M, Baroncini A. Closed suction drainages in Lower Limb Joint Arthroplasty: A level I evidence based meta-analysis. Surgeon. 2022;20:51-60. PMID: 33863671]. We aimed to examine haemoglobin (Hb) and haematocrit (Ht) levels, estimated blood loss, transfusion rate, and other aspects of supine anterolateral approach THA (ALS-THA) performed at our institution in the absence of autologous blood donation and closed suction drainage.
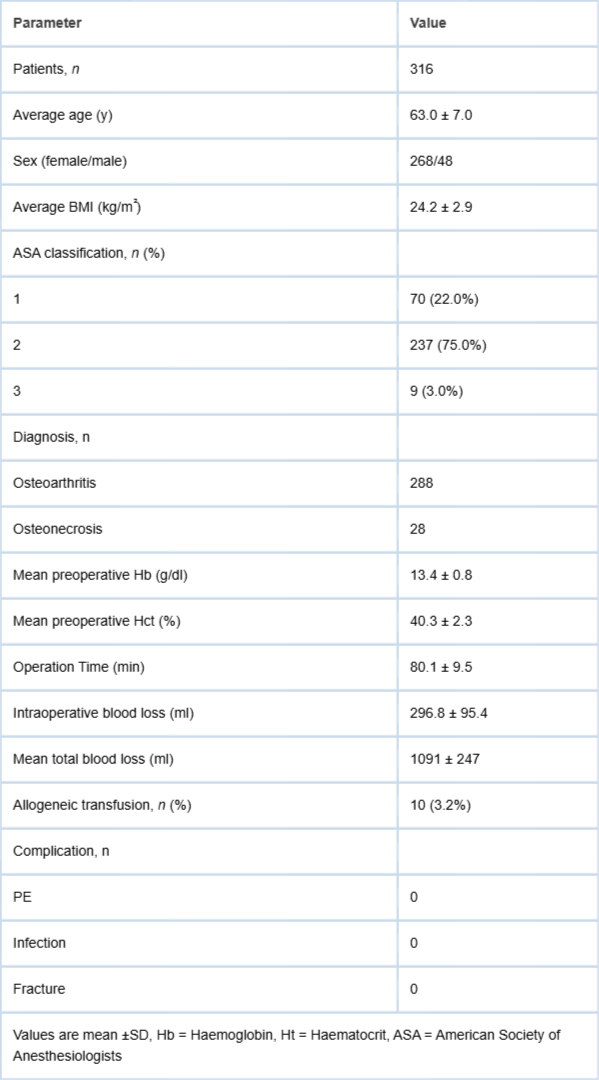
The study involved a retrospective analysis of 316 patients who underwent primary unilateral THA at our hospital from May 2021 to July 2023. The patients had preoperative Hb ≥ 10.0 g/dL. The study focused on the supine anterolateral approach THA (ALS-THA) performed without the use of autologous blood donation or closed suction drainage. The study cohort comprised 48 joints in 48 men (15.2%), and 268 joints in 268 women (84.8%). The average age was 63.0 (range: 49-85) years. The mean follow-up period for this study was approximately 1.5 years (6 months to 2.5 years). All patients underwent surgery under general anaesthesia without autologous blood donation. The target diseases included 288 cases of hip osteoarthritis and 28 cases of osteonecrosis of the femoral head (Table 1). THA performed for pseudarthrosis or deformity healing after trauma and THA performed for femoral neck fractures were excluded from the study. Surgery was performed using a short tapered-wedge stem with an anterolateral approach with patients in the supine position. Surgery was performed by three surgeons (T.H., H.F., and J.K.) with experience in THA. To prevent bleeding, all patients received an intravenous injection of tranexamic acid (1000 mg) immediately before surgery. To prevent deep vein thrombosis, all patients wore elastic stockings and were administered edoxabantsil orally for one week after surgery. In addition, a closed drain tube was not placed postoperatively in any case. For postoperative rehabilitation, the patients were allowed to get out of bed and walk as much as possible with full weight bearing from the day after surgery, with the goal of being discharged from the hospital within 10 days after surgery.
Table 1: Clinicodemographic data of patients.
Hb and Ht levels were measured preoperatively and on the first, third, and seventh postoperative days. Lower limb venous echocardiography was performed for cases with D-dimer ≥10 μg/mL on the 7th postoperative day. The estimated postoperative blood loss was calculated by measuring the circulating blood volume using Nadler’s and Gross’ formulae from the pre- and postoperative minimum Ht values [1313Nadler SB, Hidalgo JH, Bloch T. Prediction of blood volume in normal human adults. Surgery. 1962;51:224-232. PMID: 21936146,1414Gross JB. Estimating allowable blood loss: corrected for dilution. Anesthesiology. 1983;58:277-280. PMID: 6829965]. Blood transfusions were performed for patients with Hb levels below 7.5 and patients with anemia symptoms. The following factors were evaluated: Hb, Ht, C-Reactive Protein (CRP), D-dimer, and Soluble Fibrin monomer complex (SF), as well as surgical time, intraoperative blood loss, estimated postoperative blood loss, and allogeneic blood transfusion rate. We investigated the incidence of Deep Vein Thrombosis (DVT), Pulmonary Embolism (PE), infection, and fracture. Logistic regression analysis was performed targeting age, sex, blood type, height, weight, Body Mass Index (BMI), and preoperative Hb and Ht levels to examine the risk of blood transfusion. Furthermore, preoperative Hb level and the presence or absence of blood transfusion were tested using Receiver Operating Characteristic (ROC) analysis, with preoperative Hb level as the variable and blood transfusion as the outcome.
Statistical analysis
All data analysis was performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA).
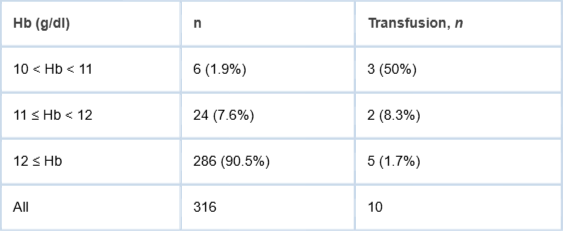
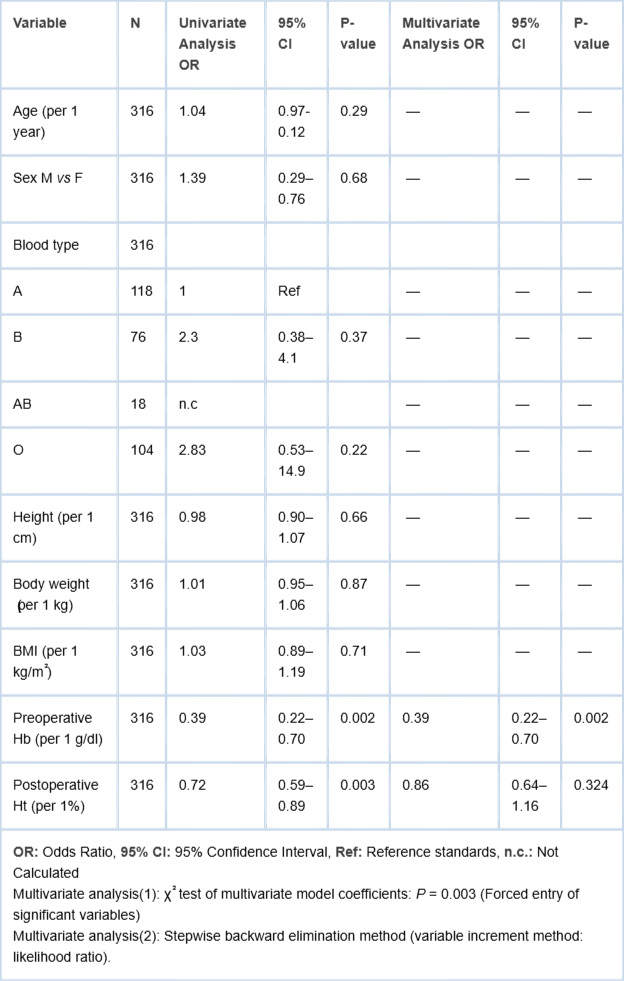
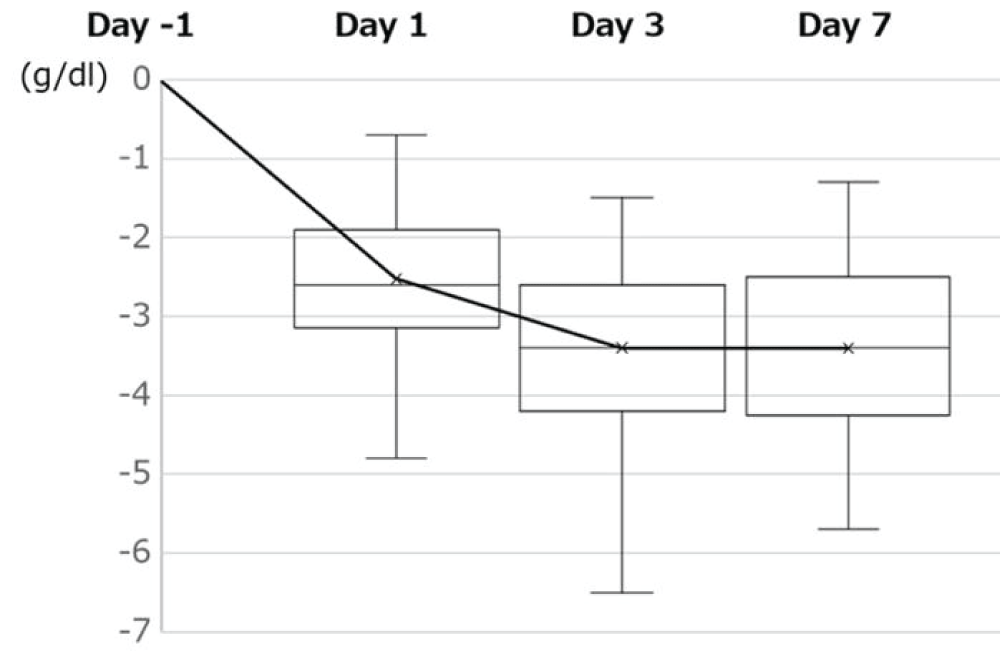
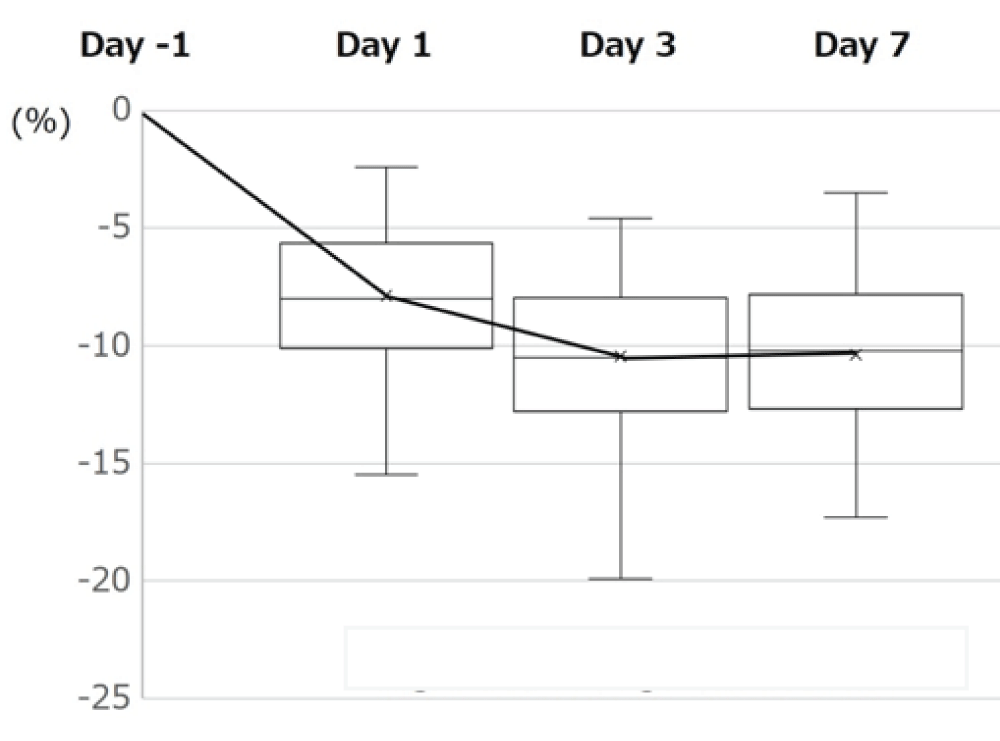
Regarding patient characteristics, the average BMI was 24.2±2.9 kg/m2, the average preoperative Hb was 13.4±0.8 g/dL, the average preoperative Ht was 40.3±2.3%. The preoperative American Society of Anesthesiologists classification was 1 in 70 patients (22.0%), 2 in 237 patients (75.0%), and 3 in 9 patients (3.0%). The average operative time was 80.1±9.5 min, the intraoperative blood loss was 296.8 ±95.4 ml, and the estimated postoperative blood loss was approximately 1091±247 ml. The blood transfusion rate in this study was 10 out of 316 cases (3.2%). Six patients (1.9%) had preoperative Hb levels ≥ 10 and < 11 g/dL, and three received blood transfusions. Twenty-four patients (7.6%) had preoperative Hb levels ≥11 g/dL and < 12 g/dL, and two received blood transfusions. A total of 286 patients (90.5%) had preoperative Hb levels >12 g/dL, and 5 required blood transfusions. The transfusion rates differed significantly among the three hemoglobin groups (Fisher’s exact test, p < 0.001). The transfusion rates were 50.0% (3/6) in patients with 10 ≤ Hb < 11 g/dL, 8.3% (2/24) in those with 11 ≤ Hb < 12 g/dL, and 1.7% (5/286) in those with Hb ≥ 12 g/dL.In pairwise comparisons, patients with 10 ≤ Hb < 11 g/dL had a significantly higher transfusion rate than those with 11 ≤ Hb < 12 g/dL and those with Hb ≥ 12 g/dL after Bonferroni correction. No significant difference was observed between the latter two groups. However, the number of patients in the 10 ≤ Hb < 11 g/dL group was small (n = 6), and therefore the results should be interpreted with caution (Table 2). There were no complications, such as symptomatic DVT or PE, infection, or fracture (Table 1). The postoperative Hb change (⊿Hb) based on the preoperative average Hb value was -2.7 ±1.3 g/dL on the first postoperative day, -3.3±0.8 g/dL on the third postoperative day, and -3.3±0.7 g/dL on the 7th postoperative day (Figure 1). The average maximum ⊿Hb (preoperative Hb - postoperative minimum Hb) was 3.3±0.8 g/dL. Changes in postoperative ⊿Hct based on the preoperative average Ht value were -7.8±2.5% on the first postoperative day, -10.5±2.4% on the third postoperative day, and -10.2±2.5% on the seventh postoperative day (Figure 2). The average maximum ⊿Ht (preoperative Ht - postoperative minimum Ht) was 11.3+2.1%. D-dimer reached a maximum value of 9.4±1.8 μg/dL one week after surgery, and SF reached a maximum value of 9.3±2.1 μg/dL on the third postoperative day. Both values peaked on the 7th postoperative day. To examine the risk of blood transfusion, we performed logistic regression analysis targeting age, sex, blood type, height, weight, BMI, preoperative Hb, and preoperative Ht. Univariate analysis showed significant differences in preoperative Hb and Ht levels. Multivariate analysis of preoperative Hb and Ht revealed a significant difference in preoperative Hb levels, with an odds ratio of 0.39 (Table 3). Increase in hemoglobin of 1 g/dL was associated with a 61% reduction in the risk of transfusion.
Table 2: Blood transfusion rates according to preoperative haemoglobin levels.
Table 3: Logistic regression analysis of blood transfusion risk factors in total hip arthroplasty.
Figure 1: Changes in ⊿Hb.
Figure 2: Changes in ⊿Htc.
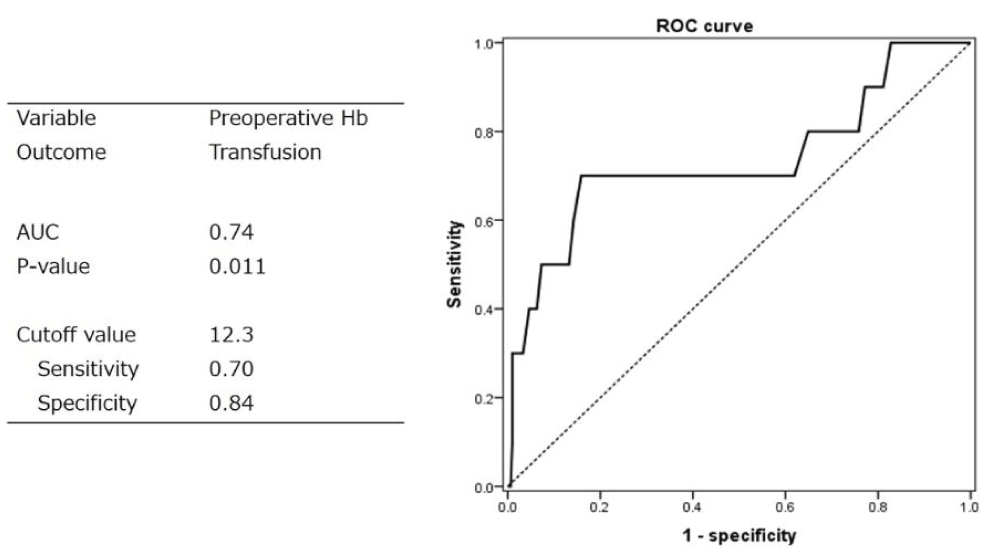
ROC analysis was performed with preoperative Hb level as the variable with blood transfusion as the outcome, and Receiver Operating Characteristic (ROC) analysis was performed. The cutoff value determined using the Youden Index method was Hb 12.3 g/dL, sensitivity 0.7, specificity 0.84, and area under the surface 0.74 (Figure 3). The results revealed that 70% of those who received a blood transfusion had a preoperative Hb ≤ 12.3 g/dL, and 84% of those who did not receive a blood transfusion had preoperative Hb ≥ 12.3 g/dL.
Figure 3: Receiver Operating Characteristic (ROC) analysis with preoperative Hb as a variable and blood transfusion as the outcome. AUC: Area under the ROC curve.
Since the 2000s, tranexamic acid administration has been shown to be effective in reducing blood loss in THA. Johansson et al. conducted a randomised, double-blind study of 100 patients who underwent THA and identified a significant difference in total blood loss, with an average of 0.97 L in the tranexamic acid group compared to 1.3 L in the placebo group. It has been reported that 8 of 47 patients (20%) in the tranexamic acid group and 23 of 53 patients (40%) in the placebo group received blood transfusions, indicating a significant difference [77Johansson T, Pettersson LG, Lisander B. Tranexamic acid in total hip arthroplasty saves blood and money: a randomized, double-blind study in 100 patients. Acta Orthop. 2005; 76: 314-319. PMID: 16156456]. Gill, et al. conducted a meta-analysis of 13 randomised clinical trials involving THA and reported that TXA administration effectively reduced intraoperative blood loss, total blood loss, and transfusion rates without increasing the risk of VTE [88Gill JB, Rosenstein A. The use of antifibrinolytic agents in total hip arthroplasty: a meta-analysis. J Arthroplasty. 2006;21:869-873. PMID: 16950041]. Tranexamic acid was also routinely administered at our hospital in patients undergoing ALS-THA.
Previously, closed suction drainage was commonly performed during THA. Closed drains reduce dead space and prevent hematomas, but they increase the risk of infection and delay rehabilitation. Since 2000, studies have shown that the use of closed suction drainage does not increase blood loss or transfusion rates [99Widman J, Jacobsson H, Larsson SA, Isacson J. No effect of drains on thepostoperative hematoma volume in hip replacement surgery. A randomized study using scintigraphy. Acta Orthop Scand. 2002;73:625-629. PMID: 12553508]. Zhou, et al. conducted a meta-analysis of 20 randomised controlled trials involving 3186 patients, comparing drainage and non-drainage groups, and reported no significant differences in the incidence of infection, blood loss, changes in Hb and Ht levels, clinical evaluations, or other complications. The authors concluded that the routine use of closed-suction drainage may have more disadvantages than advantages [1515Zhou X, Li J, Xiong Y, Jiang L, Li W, Wu L. “Do we really need closed-suction drainage in total hip arthroplasty? A meta-analysis”. Int Orthop. 2013;37:2109-2118. PMID: 23982636]. Kelly, et al. conducted a meta-analysis of 16 studies involving 2705 patients on the use of postoperative closed suction drainage in THA [1616Kelly EG, Cashman JP, Imran FH, Conroy R, O’Byrne J, et al. Systematic review and meta-analysis of closed suction drainage versus non-drainage in primary hip arthroplasty. Surg Technol Int. 2014;24:295-301. PMID: 24574017,1717Suarez JC, McNamara CA, Barksdale LC, Calvo C, Szubski R, Patel PD. Closed suction drainage has no benefits in anterior hip arthroplasty: a prospective, randomized trial. J Arthroplasty. 2016;31:1954-1958. PMID: 27062352]. The results of a meta-analysis revealed that postoperative closed suction drainage increased total blood loss and transfusion requirements but showed no significant difference in surgical site infection or haematoma formation between the two groups. They also opposed routine closed-suction drainage. At our hospital, tranexamic acid was administered preoperatively and ALS-THA was performed without closed suction drainage.
There have also been several reports of ⊿Hb in THA. Pierson, et al. reported that ΔHb in 260 patients who underwent THA was 4.0 g/dL. Surgery was performed using the posterolateral approach without drain placement or autologous blood [33Pierson JL, Hannon TJ, Earles DR. A blood conservation algorithm to reduce blood transfusions after total hip and knee arthroplasty. J Bone Joint Surg Am. 2004;87:1512-1518. PMID: 15252101]. Juan, et al. reported that ⊿Hb in 120 cases of THA was 3.0 g/dL17. Surgery was performed using the DA approach and drains were used in 59 patients. Other recent reports showed ⊿Hb values of 2.5 to 3.5 g/dL [1818Jungwirth-Weinberger A, Do HT, Krell EC, Valle AGD, Chalmers BP, Boettner F. Blood management in direct anterior versus posterior primary total hip arthroplasty using tranexamic acid: a matched cohort study. Arch Orthop Trauma Surg. 2023;143:91-95. PMID: 34152489,1919Vles GF, Corten K, Driesen R, van Elst C, Ghijselings SG. Hidden blood loss in direct anterior total hip arthroplasty: a prospective, double blind, randomized controlled trial on topical versus intravenous tranexamic acid. Musculoskelet Surg. 2021;105:267-273. PMID: 32152813]. In the present study, ⊿Hb was 3.3 g/dL, which is comparable to those in recent reports.
In a report on preoperative Hb cutoff values, Mitchell, et al. conducted a retrospective study of 558 patients who underwent posterior THA [2020Klement MR, Peres-Da-Silva A, Nickel BT, Green CL, Wellman SS, Attarian DE, et al. What Should Define Preoperative Anemia in Primary THA?. Clin Orthop Relat Res. 2017;475:2692-2693. PMID: 28786087]. In that study, the transfusion rate was 11%, and the preoperative Hb level was a risk factor for blood transfusion, with a cut-off value of 12.6 g/dL (sensitivity, 85%; specificity, 77%). In our study, the blood transfusion rate was calculated by defining patients who received blood transfusion as having a postoperative minimum Hb < 7.5 mg/dL or due to anaemia symptoms. The blood transfusion rate in this study was 10 out of 316 cases (3.2%). The ROC curve based on preoperative Hb values and whether allogeneic blood transfusion was performed, yielded a preoperative Hb cutoff value of 12.3 g/dL (sensitivity: 0.7, specificity: 0.84, area under the curve: 0.74). In our study, the transfusion rate was lower than that in previous reports, and the cutoff value was lower. It was suggested that if the preoperative Hb was ≥12.3 g/dL, there was a high probability that allogeneic blood transfusion would be unnecessary.
In 2016, Menendez, et al. reported a transfusion rate of approximately 9% in THA [2121Menendez ME, Lu N, Huybrechts KF, Ring D, Barnes CL, Ladha K, et al. Variation in use of blood transfusion in primary total hip and knee arthroplasties. J Arthroplasty. 2016;31:2757-2763. PMID: 27325367]. Recent reports on transfusion rates for anterior approaches have been reported at approximately 1% - 9% [1818Jungwirth-Weinberger A, Do HT, Krell EC, Valle AGD, Chalmers BP, Boettner F. Blood management in direct anterior versus posterior primary total hip arthroplasty using tranexamic acid: a matched cohort study. Arch Orthop Trauma Surg. 2023;143:91-95. PMID: 34152489,2222Aggarwal VK, Elbuluk A, Dundon J, Herrero C, Hernandez C, Vigdorchik JM, et al. Surgical approach significantly affects the complication rates associated with total hip arthroplasty. Bone Joint J. 2019;101:646-651. PMID: 31154834,2323Zhao HY, Kang PD, Xia YY, Shi X, Nie Y, Pei F. Comparison of early functional recovery following total hip arthroplasty using a direct anterior or posterolateral approach: a randomized controlled trial. J Arthroplasty. 2017;32:3421-3428. PMID: 28662957]. Furthermore, recent studies have reported that preoperative Patient Blood Management (PBM) reduces transfusion rates. Hourlier, et al. reported that the use of PBM protocol was associated with a zero-percent transfusion rate in a large series of consecutive patients, including those with stage 3 or 4 Chronic Kidney Disease (CKD) [2424Hourlier H, Fennema P. Application of an adjusted patient blood management protocol in patients undergoing elective total hip arthroplasty: towards a zero-percent transfusion rate in renal patients-results from an observational cohort study. J Orthop Surg Res. 2021;16:697. PMID: 34838063]. In our study, 30 patients had preoperative Hb levels < 12 g/dL, and five (16.7%) required blood transfusion. Our multivariate analysis revealed that the preoperative Hb level was most strongly associated with transfusion risk. We may further reduce the THA transfusion rate by introducing PMB.
The limitations of this study include the fact that the surgeons performing the procedure were not the same. Also, it is unclear whether the lowest Hb/Ht value is the true lowest value for the patient. Further, group comparisons between the posterior approach and drain placement groups were not possible. In this study, 84.8% of the patients were% female and 15.2% male, which constituted a significant difference. This was a retrospective cohort study presenting the outcomes of a group of patients over a certain period. This study lacked a comparison control group (e.g., patients who underwent drainage or received autologous blood transfusion), which may have influenced the observed risk of transfusion. In addition, because patients with a preoperative hemoglobin level ≤10 g/dL were excluded, the true risk of transfusion may have been underestimated. Furthermore, the relatively small number of transfusion events may have affected the robustness of the statistical analyses.
Finally, we propose that by conducting future research in patients with low preoperative Hb levels undergoing THA who receive PBM, we will be able to confirm whether the introduction of PBM leads to a reduction in blood transfusions. In my country, erythropoietin administration is covered by insurance when Hb is ≤10 mg/dL. Therefore, considerable challenges remain regarding the introduction of PMB before surgery. In addition, differences in the skill of surgeons may also play a crucial role in controlling bleeding, and it is important to establish educational tools for acquiring the requisite expertise.
This study demonstrates that the preoperative Hb level is the primary determinant of the risk of transfusion in THA. In addition, the transfusion rate was 16.7% in patients with preoperative Hb levels < 12 g/dL. Therefore, the introduction of preoperative PBM may lead to further reductions in blood transfusions.
All study participants provided written informed consent and the study protocol was approved by the appropriate ethics review board. No funding support or conflicts of interest exist for this study.
Availability of data and materials
Data presented in this study are available upon request from the corresponding author. The data were not publicly available because of the regulations of the local institutional ethics board.
Competing interests: The authors declare that there are no competing interests.
Funding: There is no funding source.
Authors’ contributions
F. and T. H. contributed to the conceptualisation, methodology, formal analysis, resources, data curation, writing-original draft preparation, writing-review and editing, and project administration; H.F. visualised the study; and T.H. supervised the study. All authors have read and agreed to the published version of the manuscript.
Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB. Ananalysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am. 1999;81:2-10. PMID: 9973048
Billote DB, Glisson SN, Green D, Wixson RL . Efficacy of preoperative autologous blood donation: analysis of blood loss and transfusion practice in total hip replacement. J Clin Anesth. 2000;12:537-542. PMID: 11137415
Pierson JL, Hannon TJ, Earles DR. A blood conservation algorithm to reduce blood transfusions after total hip and knee arthroplasty. J Bone Joint Surg Am. 2004;87:1512-1518. PMID: 15252101
Sinclair ST, Warren JA, Murray TG, Bloomfield MR, McLaughlin JP, Piuzzi NS. Blood management in total hip arthroplasty: a nationwide trend analysis from 2011 to 2018. Eur J Orthop Surg Traumatol. 2023;33:45-50. PMID: 34714392
Alvarez JC, Santiveri FX, Ramos I, Vela E, Puig L, Escolano F. Tranexamic acid reduces blood transfusion in total knee arthroplasty even when a blood conservation program is applied. Transfusion. 2008;48:519-525. PMID: 18067499
Camarasa MA, Ollé G, Serra-Prat M, Martín A, Sánchez M, Ricós P, et al. Efficacy of aminocaproic, tranexamic acids in the control of bleeding during total knee replacement: a randomized clinical trial. Br J Anaesth. 2006;96:576-582. PMID: 16531440
Johansson T, Pettersson LG, Lisander B. Tranexamic acid in total hip arthroplasty saves blood and money: a randomized, double-blind study in 100 patients. Acta Orthop. 2005; 76: 314-319. PMID: 16156456
Gill JB, Rosenstein A. The use of antifibrinolytic agents in total hip arthroplasty: a meta-analysis. J Arthroplasty. 2006;21:869-873. PMID: 16950041
Widman J, Jacobsson H, Larsson SA, Isacson J. No effect of drains on thepostoperative hematoma volume in hip replacement surgery. A randomized study using scintigraphy. Acta Orthop Scand. 2002;73:625-629. PMID: 12553508
Parker MJ, Roberts CP, Hay D. Closed suction drainage for hip and knee arthroplasty. A meta-analysis. J Bone Joint Surg Am.2004;86:1146-1152. PMID: 15173286
Walmsley PJ, Kelly MB, Hill RM, Brenkel I. A prospective, randomised, controlled trial of the use of drains in total hip arthroplasty. J Bone Joint Surg Br. 2005;87:1397-1401. PMID: 16189315
Migliorini F, Maffulli N, Betsch M, Eschweiler J, Tingart M, Baroncini A. Closed suction drainages in Lower Limb Joint Arthroplasty: A level I evidence based meta-analysis. Surgeon. 2022;20:51-60. PMID: 33863671
Nadler SB, Hidalgo JH, Bloch T. Prediction of blood volume in normal human adults. Surgery. 1962;51:224-232. PMID: 21936146
Zhou X, Li J, Xiong Y, Jiang L, Li W, Wu L. “Do we really need closed-suction drainage in total hip arthroplasty? A meta-analysis”. Int Orthop. 2013;37:2109-2118. PMID: 23982636
Kelly EG, Cashman JP, Imran FH, Conroy R, O’Byrne J, et al. Systematic review and meta-analysis of closed suction drainage versus non-drainage in primary hip arthroplasty. Surg Technol Int. 2014;24:295-301. PMID: 24574017
Suarez JC, McNamara CA, Barksdale LC, Calvo C, Szubski R, Patel PD. Closed suction drainage has no benefits in anterior hip arthroplasty: a prospective, randomized trial. J Arthroplasty. 2016;31:1954-1958. PMID: 27062352
Jungwirth-Weinberger A, Do HT, Krell EC, Valle AGD, Chalmers BP, Boettner F. Blood management in direct anterior versus posterior primary total hip arthroplasty using tranexamic acid: a matched cohort study. Arch Orthop Trauma Surg. 2023;143:91-95. PMID: 34152489
Vles GF, Corten K, Driesen R, van Elst C, Ghijselings SG. Hidden blood loss in direct anterior total hip arthroplasty: a prospective, double blind, randomized controlled trial on topical versus intravenous tranexamic acid. Musculoskelet Surg. 2021;105:267-273. PMID: 32152813
Klement MR, Peres-Da-Silva A, Nickel BT, Green CL, Wellman SS, Attarian DE, et al. What Should Define Preoperative Anemia in Primary THA?. Clin Orthop Relat Res. 2017;475:2692-2693. PMID: 28786087
Menendez ME, Lu N, Huybrechts KF, Ring D, Barnes CL, Ladha K, et al. Variation in use of blood transfusion in primary total hip and knee arthroplasties. J Arthroplasty. 2016;31:2757-2763. PMID: 27325367
Aggarwal VK, Elbuluk A, Dundon J, Herrero C, Hernandez C, Vigdorchik JM, et al. Surgical approach significantly affects the complication rates associated with total hip arthroplasty. Bone Joint J. 2019;101:646-651. PMID: 31154834
Zhao HY, Kang PD, Xia YY, Shi X, Nie Y, Pei F. Comparison of early functional recovery following total hip arthroplasty using a direct anterior or posterolateral approach: a randomized controlled trial. J Arthroplasty. 2017;32:3421-3428. PMID: 28662957
Hourlier H, Fennema P. Application of an adjusted patient blood management protocol in patients undergoing elective total hip arthroplasty: towards a zero-percent transfusion rate in renal patients-results from an observational cohort study. J Orthop Surg Res. 2021;16:697. PMID: 34838063
Fujimaki H. Transfusion Risk in Anterolateral Total Hip Arthroplasty without closed Suction Drainage and Autologous Blood Donation. IgMin Res. May 11, 2026; 4(4): 163-168. IgMin ID: igmin341; DOI:10.61927/igmin341; Available at: igmin.link/p341
How to cite this article: Fujimaki H. Transfusion Risk in Anterolateral Total Hip Arthroplasty without closed Suction Drainage and Autologous Blood Donation. IgMin Res. May 11, 2026; 4(4): 163-168. IgMin ID: igmin341; DOI:10.61927/igmin341; Available at: igmin.link/p341
Copyright: 2026 Fujimaki H. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Table 2: Blood transfusion rates according to preoperative ...
Table 3: Logistic regression analysis of blood transfusion ...
Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB. Ananalysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am. 1999;81:2-10. PMID: 9973048
Billote DB, Glisson SN, Green D, Wixson RL . Efficacy of preoperative autologous blood donation: analysis of blood loss and transfusion practice in total hip replacement. J Clin Anesth. 2000;12:537-542. PMID: 11137415
Pierson JL, Hannon TJ, Earles DR. A blood conservation algorithm to reduce blood transfusions after total hip and knee arthroplasty. J Bone Joint Surg Am. 2004;87:1512-1518. PMID: 15252101
Sinclair ST, Warren JA, Murray TG, Bloomfield MR, McLaughlin JP, Piuzzi NS. Blood management in total hip arthroplasty: a nationwide trend analysis from 2011 to 2018. Eur J Orthop Surg Traumatol. 2023;33:45-50. PMID: 34714392
Alvarez JC, Santiveri FX, Ramos I, Vela E, Puig L, Escolano F. Tranexamic acid reduces blood transfusion in total knee arthroplasty even when a blood conservation program is applied. Transfusion. 2008;48:519-525. PMID: 18067499
Camarasa MA, Ollé G, Serra-Prat M, Martín A, Sánchez M, Ricós P, et al. Efficacy of aminocaproic, tranexamic acids in the control of bleeding during total knee replacement: a randomized clinical trial. Br J Anaesth. 2006;96:576-582. PMID: 16531440
Johansson T, Pettersson LG, Lisander B. Tranexamic acid in total hip arthroplasty saves blood and money: a randomized, double-blind study in 100 patients. Acta Orthop. 2005; 76: 314-319. PMID: 16156456
Gill JB, Rosenstein A. The use of antifibrinolytic agents in total hip arthroplasty: a meta-analysis. J Arthroplasty. 2006;21:869-873. PMID: 16950041
Widman J, Jacobsson H, Larsson SA, Isacson J. No effect of drains on thepostoperative hematoma volume in hip replacement surgery. A randomized study using scintigraphy. Acta Orthop Scand. 2002;73:625-629. PMID: 12553508
Parker MJ, Roberts CP, Hay D. Closed suction drainage for hip and knee arthroplasty. A meta-analysis. J Bone Joint Surg Am.2004;86:1146-1152. PMID: 15173286
Walmsley PJ, Kelly MB, Hill RM, Brenkel I. A prospective, randomised, controlled trial of the use of drains in total hip arthroplasty. J Bone Joint Surg Br. 2005;87:1397-1401. PMID: 16189315
Migliorini F, Maffulli N, Betsch M, Eschweiler J, Tingart M, Baroncini A. Closed suction drainages in Lower Limb Joint Arthroplasty: A level I evidence based meta-analysis. Surgeon. 2022;20:51-60. PMID: 33863671
Nadler SB, Hidalgo JH, Bloch T. Prediction of blood volume in normal human adults. Surgery. 1962;51:224-232. PMID: 21936146
Zhou X, Li J, Xiong Y, Jiang L, Li W, Wu L. “Do we really need closed-suction drainage in total hip arthroplasty? A meta-analysis”. Int Orthop. 2013;37:2109-2118. PMID: 23982636
Kelly EG, Cashman JP, Imran FH, Conroy R, O’Byrne J, et al. Systematic review and meta-analysis of closed suction drainage versus non-drainage in primary hip arthroplasty. Surg Technol Int. 2014;24:295-301. PMID: 24574017
Suarez JC, McNamara CA, Barksdale LC, Calvo C, Szubski R, Patel PD. Closed suction drainage has no benefits in anterior hip arthroplasty: a prospective, randomized trial. J Arthroplasty. 2016;31:1954-1958. PMID: 27062352
Jungwirth-Weinberger A, Do HT, Krell EC, Valle AGD, Chalmers BP, Boettner F. Blood management in direct anterior versus posterior primary total hip arthroplasty using tranexamic acid: a matched cohort study. Arch Orthop Trauma Surg. 2023;143:91-95. PMID: 34152489
Vles GF, Corten K, Driesen R, van Elst C, Ghijselings SG. Hidden blood loss in direct anterior total hip arthroplasty: a prospective, double blind, randomized controlled trial on topical versus intravenous tranexamic acid. Musculoskelet Surg. 2021;105:267-273. PMID: 32152813
Klement MR, Peres-Da-Silva A, Nickel BT, Green CL, Wellman SS, Attarian DE, et al. What Should Define Preoperative Anemia in Primary THA?. Clin Orthop Relat Res. 2017;475:2692-2693. PMID: 28786087
Menendez ME, Lu N, Huybrechts KF, Ring D, Barnes CL, Ladha K, et al. Variation in use of blood transfusion in primary total hip and knee arthroplasties. J Arthroplasty. 2016;31:2757-2763. PMID: 27325367
Aggarwal VK, Elbuluk A, Dundon J, Herrero C, Hernandez C, Vigdorchik JM, et al. Surgical approach significantly affects the complication rates associated with total hip arthroplasty. Bone Joint J. 2019;101:646-651. PMID: 31154834
Zhao HY, Kang PD, Xia YY, Shi X, Nie Y, Pei F. Comparison of early functional recovery following total hip arthroplasty using a direct anterior or posterolateral approach: a randomized controlled trial. J Arthroplasty. 2017;32:3421-3428. PMID: 28662957
Hourlier H, Fennema P. Application of an adjusted patient blood management protocol in patients undergoing elective total hip arthroplasty: towards a zero-percent transfusion rate in renal patients-results from an observational cohort study. J Orthop Surg Res. 2021;16:697. PMID: 34838063


 Scan and get link
Scan and get link